 Zoe Moula
Zoe Moula Joanne Powell
Joanne Powell Shirley Brocklehurst
Shirley Brocklehurst Vicky Karkou
Vicky Karkou- 1Imperial College London, London, United Kingdom
- 2Faculty of Health, Social Care & Medicine and Faculty of Psychology, Edge Hill University, Ormskirk, United Kingdom
Background: Schools have been increasingly employing dance movement psychotherapists to support children cope with daily worries and stress, express and understand their emotions, develop self-awareness and self-esteem. However, evidence on the impact of dance movement psychotherapy as a tool for prevention of mental health difficulties in childhood remains limited.
Methods: Sixteen children (aged 7–9) with mild emotional and behavioral difficulties from two primary schools were randomly assigned to a Dance Movement Psychotherapy (DMP) intervention or to a waiting list, within a larger pilot cross-over randomized controlled study which aimed to (a) test whether all elements of study design can work together and run smoothly in a full-scale RCT; and (b) investigate the effectiveness of arts therapies in improving children’s health related quality of life (HRQOL; EQ-5D-Y), wellbeing and life functioning (Child Outcome Rating Scale; CORS), emotional and behavioral difficulties (Strengths and Difficulties Questionnaire; SDQ), and duration of sleep (Fitbits). The therapeutic process was also evaluated through interviews with children, participant observations, the Children’s Session Rating Scale (CSRS), and ratings of adherence to the therapeutic protocol.
Results: The findings indicated that DMP led to improvements in children’s life functioning, wellbeing, duration of sleep, emotional and behavioral difficulties, but not in quality of life. The improvements were maintained at the follow-up stages, up to 6 months post-intervention. Interviews with children also suggested positive outcomes, such as self-expression; emotional regulation; mastery and acceptance of emotions; improved self-confidence and self-esteem; reduced stress; and development of positive relationships. However, children would have preferred smaller groups and longer sessions.
Conclusion: This study indicated that all outcome measures would be suitable for inclusion in a larger randomized controlled trial, though the EQ-5D-Y is not recommended as a stand-alone measure due to its lack of sensitivity and specificity for young participants. The adherence to the therapeutic protocol ratings differed between children and adults, highlighting the need to include children’s voice in future research. Strategies are also proposed of how to conduct randomization of participants in ways that do not hinder the therapeutic process.
Introduction
Mental health provision for children in schools
In the United Kingdom, one in five children (equating to 1.1 million) reported feeling unhappy with their lives since the COVID-19 crisis (Children’s Commissioner, 2021). Clinically significant mental health conditions have increased by 50%, while two thirds of primary school children have experienced social isolation and loneliness; also a 50% increase compared to pre-COVID-19 (Children’s Commissioner, 2021). Furthermore, although the number of domestic abuse rose by at least 30%, the number of children coming to the attention of services has fallen dramatically (Children’s Society, 2020). It is therefore not surprising that in a survey of 2,438 children and young people (Young Minds, 2021), approximately 70% said that pandemic will have a long-term negative effect on their mental health.
The World Health Organisation (WHO) (2004) proposes that mental health promotion should be integrated into the school curriculum, reaching children who might not otherwise obtain help. Although school mental health provision varies across countries, the European Union Dataprev project found that over the past 25 years there has been a significant increase in large-scale school mental health programs (Weare and Nind, 2011; Patalay et al., 2017). Having daily contact with children and their families, schools are a key entry point to community-based mental health provision (Stephan et al., 2007; Jané-Llopis and Braddick, 2008; Caan et al., 2014). Their remit as educational institutions helps to reduce stigma, increases inclusivity, while accessing supportive networks of peers, teachers, healthcare professionals, and parents (Kavanagh et al., 2009; Greenberg, 2010). Furthermore, school-based counselors and psychotherapists can streamline the referral process and target children experiencing barriers due to lack of transportation, parent work schedules, funding, and inadequate treatment from other sources (Capp, 2015).
Nevertheless, a major challenge for school mental health services is that the focus relies heavily on the treatment of severe difficulties or disorders, whereas early detection and prevention might be equally important (The World Health Organisation [WHO], 2004; Goldie et al., 2016). When opportunities for prevention are missed, chances are increasing for children to drop out of school, self-harm, become aggressive, violent, or even suicidal. In the United Kingdom, it is estimated that 7,000 children are being excluded annually (equivalent to 35 children/day) while 1,300 of these exclusions come from primary schools (Children’s Commissioner for England, 2017). This might be because more than 70% of children lack supportive services at a sufficiently early age (Children’s Society, 2018), 30% of referrals are turned away and waiting lists can take up to a year (Children’s Commissioner for England, 2017). Such delays in addressing children’s needs have long-lasting and potentially irreversible negative effects, highlighting the importance of support at the early stages of children’s education.
Dance movement psychotherapy for children in schools
The UK Professional Association for Dance Movement Psychotherapy [ADMPUK] (2013) has defined DMP as “a relational process in which client/s and therapist engage creatively using body movement and dance to assist integration of emotional, cognitive, physical, social and spiritual aspects of self” (p. 1). Schools are increasingly employing DMP practitioners to support children cope with stress and worries, express and understand their emotions, develop self-awareness and self-esteem (Karkou, 2010; Moula et al., 2020b; Karkou et al., 2022). Embedding DMP within the educational system, may feasibly, address children’s emerging needs and have a positive impact on their wellbeing, bridging the gap between health and education.
DMP is especially important for children who might not wish, or are unable, to verbalize their thoughts and emotions, especially under stressful circumstances (Moula et al., 2019). This is because DMP emphasizes the externalization of bodily felt emotions in creative ways, aiming to assist children process difficult feelings and integrate new self-soothing strategies (Meekums, 2008). The connection between motion and emotion is integrative in DMP, as movement has an emotional content and the expression of this content forms the basis for the therapeutic process (Berger, 1972; Johnson, 1995). As such, movement serves as an agent of expression of inner tensions and distress and can become a container for old and, as the therapy progresses, of new experiences (Frizzell, 2006). When DMP is delivered to children, some of the key goals include, but are not limited to: understanding and managing difficulties which may interrupt learning; social interaction skills; emotional, physical, and mental integration; self-expression; communication; self-awareness; empathy; self-esteem and self-confidence (Eke and Gent, 2010).
Evidence-based dance movement psychotherapy for children and young people
Current studies with children and young people showed that DMP can support children with a range of social, emotional, and behavioral difficulties (Goodgame, 2007; Eke and Gent, 2010; Ballard et al., 2014; Moula et al., 2020a). In terms of behavioral difficulties, DMP allows children to develop problem-solving abilities and gain methods of self-control, preventing underlying forms of aggression from being escalated into more disruptive behaviors (Koshland et al., 2004; Koolaee et al., 2014). Preliminary studies have also highlighted the value of DMP for children with ADHD (Grönlund et al., 2005; Redman, 2007), depression (Jeong et al., 2005), and learning difficulties (Lamond, 2010; Mullane and Dunphy, 2017; Unkovich et al., 2017). The impact of DMP is extending to children experiencing stressful events, such as immigration (Bareka et al., 2019; Grasser et al., 2019; Dieterich-Hartwell et al., 2020), pandemics and lockdowns (Muhs, 2021; Shuper-Engelhard and Furlager, 2021). A current systematic review has also highlighted the contribution of DMP for the wellbeing of children with ASD (Aithal et al., 2021). Furthermore, DMP had been used with children and young people in pediatric settings (Zilius, 2010) and psychiatric clinics (Erfer and Ziv, 2006; Anderson et al., 2014) addressing more complex difficulties.
However, what is missing from current evidence is the provision of DMP for prevention and resilience, rather than for treatment purposes for this age group. Existing research and practice in creative psychotherapies is based on children who have been diagnosed with a disorder or disability (Malchiodi, 2012). When existing research addresses prevention, it also tends to focus on older population. A systematic review on school-based creative psychotherapies as a tool of prevention of mental health difficulties (Moula et al., 2019) identified only two eligible DMP studies (Koshland et al., 2004; Abdulazeem, 2014). The former included children with disabilities, while the latter focused on violence prevention. No study looked at DMP with children in mainstream primary education with emotional and behavioral difficulties as a preventive intervention before developing mental health issues. The current study aimed to address this gap, by administering a DMP intervention in children with mild emotional and behavioral difficulties in a school-based setting.
Aims and objectives
This study was part of a pilot cross-over randomized controlled study delivering arts therapies across primary schools in the Northwest of England, specifically, art therapy, music therapy, dramatherapy, and dance movement psychotherapy. The design of the pilot was grounded on a systematic review (Moula et al., 2020a), which informed the development of the sessions, choice of outcome measures and research methods, while a full account of the study protocol has been published elsewhere (Moula et al., 2019). The primary aim of the pilot was to test whether all components of the study design (e.g., recruitment, randomization, outcome measures, follow-up) can work together and run smoothly in a full-scale RCT. The present article presents a sub-study of this pilot and is focused specifically on the process and outcome evaluation of the DMP intervention. As such, the research questions of this sub-study are:
1. What are the outcomes of DMP as evaluated through:
a) verbal and non-verbal expressions relating to children’s feelings and thoughts on their wellbeing;
b) self-reported standardized outcome measures relating to quality of life, wellbeing, and life functioning;
c) biomarkers relating to children’s duration of sleep?
2. To what extent the DMP intervention adhered to the therapeutic model?
Methodology
Methodological positioning
Given the complexity of health difficulties, social interventions require data collection from various perspectives and methods (Johnson et al., 2007; Creswell and Plano Clark, 2017). In this study, mixed-methods were used to evaluate the DMP process and outcomes from children’s experiences and standardized measures. This approach is philosophically underpinned by pragmatism (Howe, 1988; Creswell, 2014). Pragmatism embraces both the positivist/postpositivist and constructive paradigms aiming to gain a comprehensive understanding of the research problem both from quantitative (measured facts) and qualitative methods (personal experiences) (Onwuegbuzie and Johnson, 2006; Brierley, 2017). Epistemologically, there are times during the research design that an objective stance is adopted using standardized measures, while at other times a subjective approach is followed through attempting to understand participants’ perceived realities (Teddlie and Tashakkori, 2009) and thus, producing socially useful knowledge (Yvonne Feilzer, 2010).
Participants
Sixteen children who experienced mild emotional and behavioral difficulties were recruited from two primary schools across the Northwest of England. The eligibility criteria for participation are presented in Table 1. Half of the children were assigned to the DMP intervention group immediately after randomization, while the other half acted as control group in the beginning and received the DMP intervention 3 months later (waiting list). Detailed information about the randomization method and sample size calculations are provided in the study protocol (Moula et al., 2019). The number of children who were recruited for the DMP intervention was small because this was a sub-study of a larger pilot study (Moula et al., 2020b).
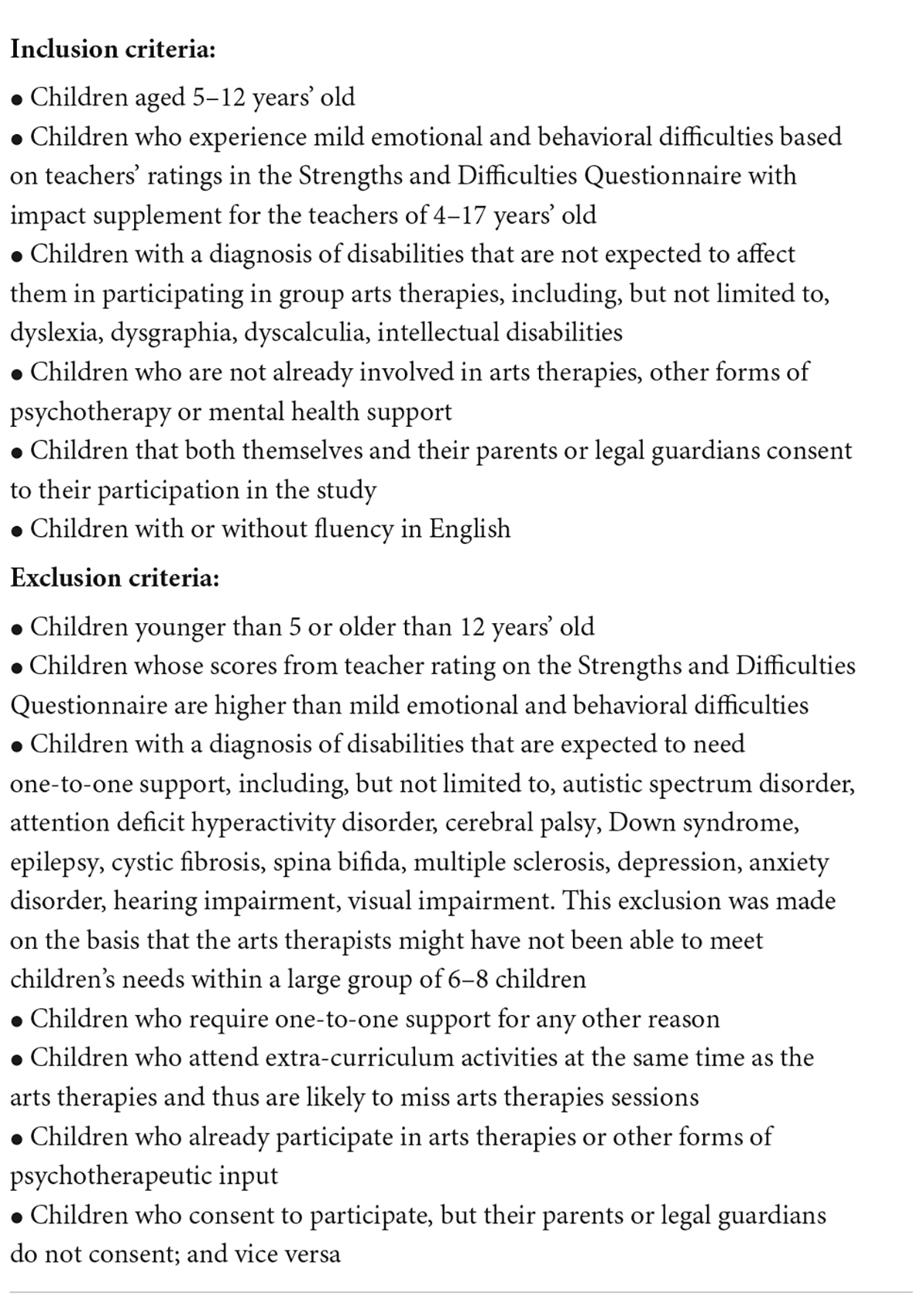
Table 1. Eligibility criteria.
For the first cohort, four girls and four boys (aged 8–9) were selected through a random number generator software. However, two boys withdrew their participation before the beginning of the sessions on the basis that “dance is not for boys.” Following their withdrawal, the other two boys expressed that they would feel uncomfortable and embarrassed if they were surrounded by girls and they decided to withdraw as well. Following discussions with the class teachers, we decided to recruit only girls for the first cohort of DMP. For the second cohort, four girls and four boys were recruited (aged 7–8). However, we emphasized that the sessions would be focused on movement, rather than on dance, and there were no withdrawals. As such, the final sample who participated in DMP consisted of 12 girls and four boys.
Dance movement psychotherapy intervention
DMP was delivered 1 h weekly, across eight consecutive weeks. Each DMP session was focused on a specific topic and therapeutic goal (Figure 1 and Table 2; see also Moula et al., 2019; Moula, 2020), based on existing evidence of previous interventions in arts therapies (Moula et al., 2020a), the Arts for the Blues model developed for adults with depression (Omylinska-Thurston et al., 2020) and the wider literature in school-based arts therapies (Karkou, 2010). It also drew on DMP theory and practice and the work of Marian Chace in particular (Chaiklin and Schmais, 1986).
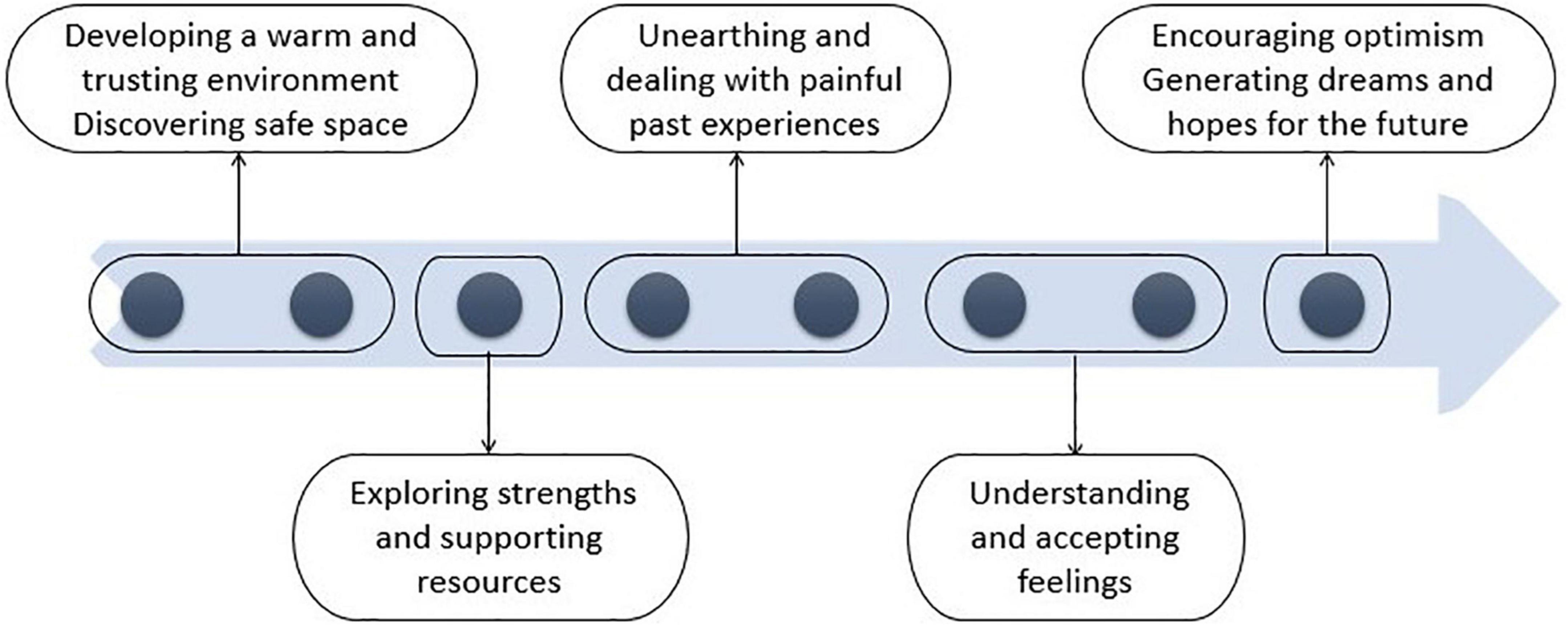
Figure 1. Therapeutic model.
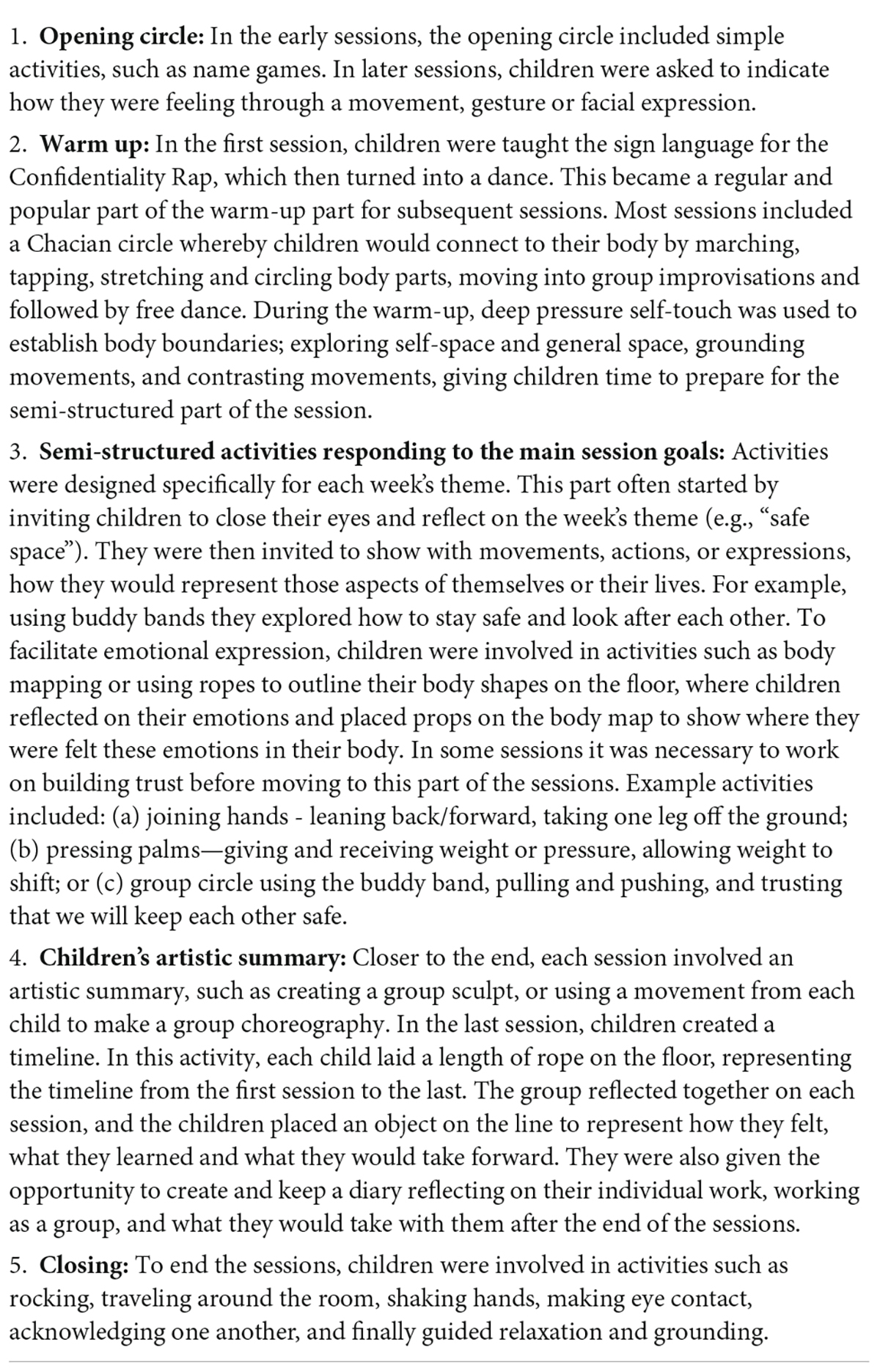
Table 2. Session structure and activities.
The DMP (SB) was trained on the protocol application and was encouraged to make her own clinical judgments moderating the session structure when needed. The DMP has been teaching dance and movement for over 45 years. She was trained and qualified as DMP 10 years ago and working as DMP since then. The protocol was used to evaluate whether the sessions adhered to the therapeutic model, and modifications were recorded for fidelity.
Data collection and analysis
The outcome evaluation was completed by interviews, questionnaires, and biomarkers (FitBits). The process evaluation was completed by participant observations, ratings of adherence to the therapeutic protocol, and children’s session ratings. A flowchart of the procedure is presented in Figure 2.
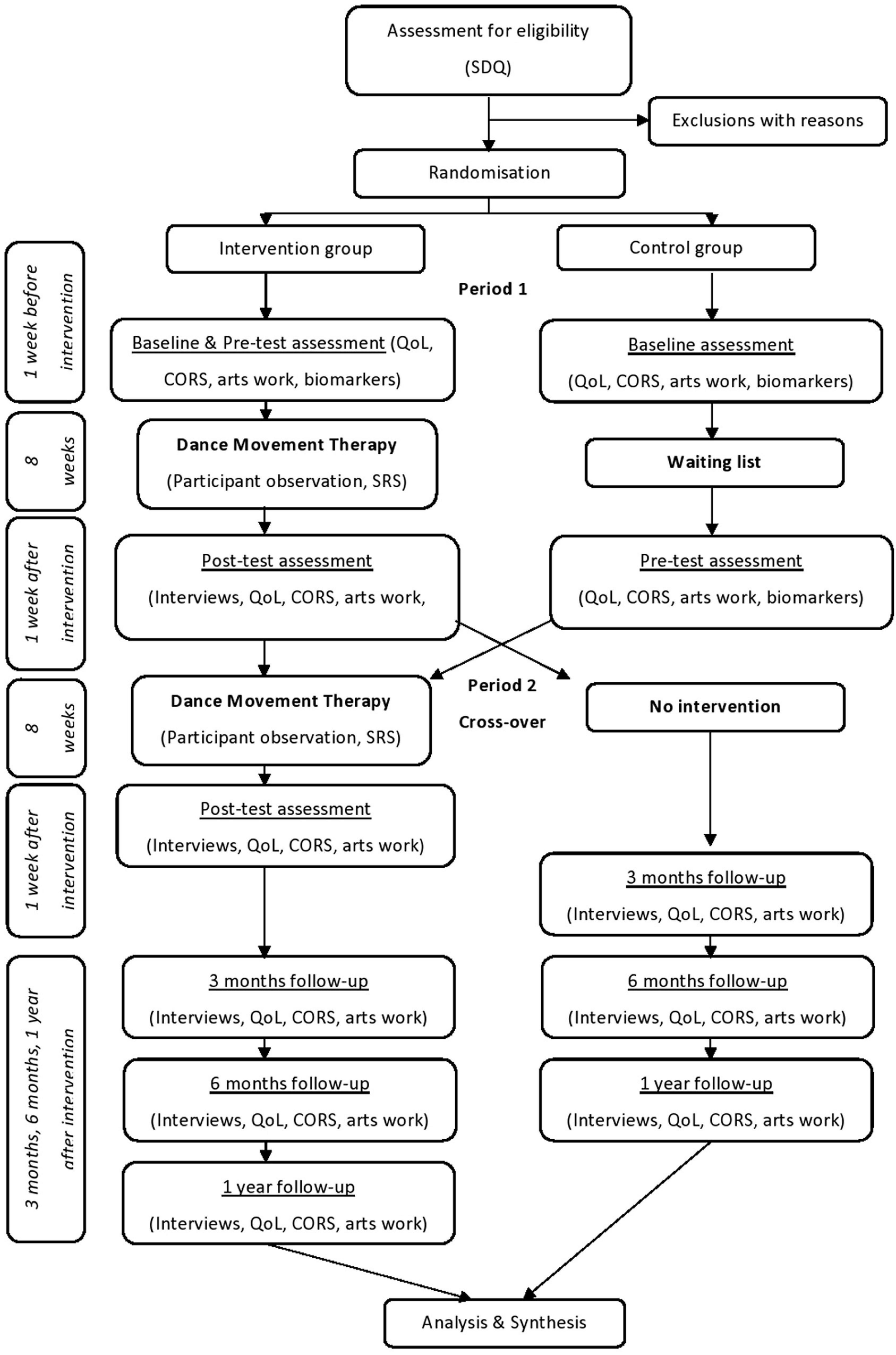
Figure 2. Procedure flowchart.
Interviews
Semi-structured one-to-one interviews were conducted at the end of the intervention to understand children’s perspectives regarding what they found helpful or unhelpful and what they enjoyed or did not enjoy. To facilitate memory retrieval, 1-2 photographs from each session were selected and showed to the children. The interviews were analyzed through reflexive thematic analysis (Braun and Clarke, 2006). To minimize power imbalance and avoid misinterpretations of children’s views, member cross-checking was employed (Brooks et al., 2017). All tentative interpretations were made available to children to express whether they represented their own viewpoints and to evaluate their accuracy (Atkinson et al., 2003). The supervisory team (VK, JP) also reviewed the interpretations and provided further insights. Both methods contributed to credibility improvements (Higgins and Green, 2011).
Adherence to therapeutic protocol
The lead researcher (ZM) was a participant observer in all sessions. At the end of each session, the researcher (ZM) and DMP (SB) rated the adherence to the therapeutic protocol and recorded any changes for fidelity purposes. Participant observation was supported by video recordings, allowing us to capture simultaneous complex interactions and observe events retrospectively (Asan and Montague, 2014). A rating was given for each of the 10 therapeutic principles by the therapist (Rater A) and the researcher (Rater B). The agreement between raters was assessed using the Bland-Altman plot system (Bland and Altman, 1986). This allowed the identification of systematic differences between the raters, which were classed as “fixed bias” or outliers. The mean score was calculated (A + B/2) along with the difference between rater scores (A - B). The overall degree of adherence from both raters estimated the inter-rater reliability. By exploring the level of intersubjectivity, this method improved the dependability of the findings (Higgins and Green, 2011).
Biomarkers
Biomarkers (FitBits) were used to capture changes in children’s duration of sleep. Children wore the Fitbits for 3 days, 1 week before and 1 week after DMP. The number of minutes asleep was calculated as the total number of minutes asleep minus the number of active minutes during the night. This calculation provided an overall measure of sleep duration, recorded in minutes. Duration of sleep was averaged across the 3 days pre-intervention and 3 days post-intervention.
Questionnaires
All children were administered a standardized battery of tests, and one questionnaire was administered to teachers. The child-reported questionnaires were the: Quality of Life for Children (EQ-5D-Y) (Wille et al., 2010); Child Outcome Rating Scale (CORS) (Low et al., 2012); Child Session Rating Scale (CSRS) (Low et al., 2012). The teacher-reported questionnaire was the Strengths and Difficulties Questionnaire with impact supplement (SDQ) (Goodman, 2001). A summary of all measures is presented below, while the study protocol (Moula et al., 2019) provides a more detailed description.
The Quality-of-Life scale for Children (EQ-5D-Y) (Wille et al., 2010) reflects young people’s own judgments of their health-related quality-of-life. It includes dimensions of activity level, self-care, doing usual activities, experiencing pain or discomfort, and feeling worried, sad, or unhappy. Test–retest reliability ranges between 69.8 and 99.7% (Ravens-Sieberer et al., 2010). Kappa coefficients reach up to 0.67, while the correlation coefficients with other measures of self-rated health indicate convergent validity up to r = –0.56 (Ravens-Sieberer et al., 2010).
The Child Outcome Rating Scale (CORS) (Low et al., 2012) evaluates areas of life functioning and wellbeing that might change following a therapeutic intervention. It includes individual wellbeing, interpersonal wellbeing, social wellbeing, and overall wellbeing. Research found moderate to high reliability (Bringhurst et al., 2006), moderate test-retest reliability (Bringhurst et al., 2006), and moderately strong concurrent validity with longer, more established measures of treatment outcome and therapeutic alliance (Miller et al., 2003; Bringhurst et al., 2006).
The Child Session Rating Scale (CSRS) (Low et al., 2012) assesses key dimensions of effective therapeutic relationships and children’s feedback on therapeutic progress. The CSRS was administered at the end of each session to get real time feedback from children so that any alliance difficulties could be identified and addressed (Miller et al., 2003). Existing research has demonstrated good reliability, test re-test reliability, and concurrent validity (Miller et al., 2003; Campbell and Hemsley, 2009).
The Strengths and Difficulties Questionnaire (SDQ) (Goodman, 2001) with impact supplement for teachers is an emotional and behavioral screening tool. The impact supplement examines the nature of difficulties, such as burden to others, social impairment, chronicity and distress. Existing evidence suggests strong internal consistency (Yao et al., 2009); moderate test-retest reliability (Yao et al., 2009); good concurrent validity (Muris et al., 2003); and good discriminant validity (Lundh et al., 2008).
IBM’s SPSS (version 25) was used for calculating means and standard deviations in the above questionnaires. Descriptives, including means and standard deviations, for all the variables in the study are presented and discussed within the results. Descriptives for the CSRS across the eight sessions as well as CORS and HRQOL at follow-up points (3- and 6 months post-intervention) are also presented.
Results
Context of dance movement psychotherapy provision in two schools
In the first school, eight children were selected from two classes (aged 8–9). However, two boys decided that “dance is not for boys” and withdrew. Following this, the other two boys expressed that they would feel uncomfortable being surrounded by girls, and they also withdrew. We therefore recruited eight girls, as other boys would feel embarrassed to participate at this stage. In this first school, there was a need for a safe and private environment that was lacking. There were frequent interruptions while the safeguarding officer required that a permanent member of staff should observe every session. However, the presence of an external non-participating observer impacted on the group who hesitated to share experiences, feelings, or thoughts in front of them. Following the first cohort’s completion, we decided to terminate the collaboration with this school.
The second cohort started in a new school, where a safe and private environment was secured this time. Eight children from two classes were recruited (aged 8–10). The study was presented as “movement therapy” to avoid dropouts from boys; there were no dropouts. Although privacy and safety were ensured, the hall was particularly spacious, requiring extra effort to contain the group. In addition, some children required attention regarding their listening skills, which created challenges for the therapeutic process. As a result, the therapist needed to modify the intervention to meet these needs as presented in the ratings of adherence to the therapeutic protocol below.
Qualitative findings
The interviews revealed that the activities that children enjoyed the most were: (a) experimenting with different fabrics and materials (e.g., scarfs, parachutes); (b) stories and role-playing; (c) mindfulness techniques (e.g., deep breathing); (d) exploring their safe space; and (e) identifying their strengths. These activities offered to children space to work individually as well as being part of the group. They also encouraged children to treat each other with kindness and respect the process of emotional sharing within a safe and non-judgmental environment. For example, one child said that:
“It was really good to share what we felt through our movements, you know, that we could share anything we feel […] this was our safe space”
Particularly the “Confidentiality Rap,” which was the first song of every session, was children’s favorite song because it reminded them that anything that was shared in the group was confidential. For example:
“I loved the song [Confidentiality Rap], my favourite part ‘what we say in the group, stays in the group, it’s confidential […] it was just to make sure that we are all protected”
The aspects of DMP that children found most helpful were being part of a team, looking after each other, and knowing that there was someone to speak to when they needed support. As a child said:
“I was helping others to feel better, some people can get upset very easily and it helped me to understand that sometimes they don’t mean it and they feel sorry. I think it helped us to become better friends”
Furthermore, children mentioned that DMP had a calming effect on them, especially when they experienced frustration and/or when they were dealing with uncomfortable situations:
“When I felt upset it helped me calm down […]. I’m fighting less with my brother now and I can control my anger better”
“When I am frustrated, I know that there are better ways to do it than being mad at other people when they haven’t really done anything and it’s not their fault”
Although there were no activities that children found unhelpful or did not enjoy, there were some aspects of the sessions that most children did not enjoy, specifically the arguments and the lack of listening. Even sensing lack of listening from one member was enough to interfere with the therapeutic process and prevent others from sharing. As a child said:
“I didn’t like shouting at each other, I would prefer smaller groups maybe like five because when we argue we lose time and it’s not fun”
As discussed below and as children recommended, working with smaller groups could improve children’s experience and better facilitate the therapeutic process.
Quantitative findings
Child outcome rating scale and health related quality of life
Table 3 shows the means and standard deviations for CORS and HRQOL post-intervention and at follow-up (i.e., 3-, and 6-months post-intervention) for those that took part in the intervention (N = 16) and from the control intervention (N = 8) as well as the total sample (N = 24).
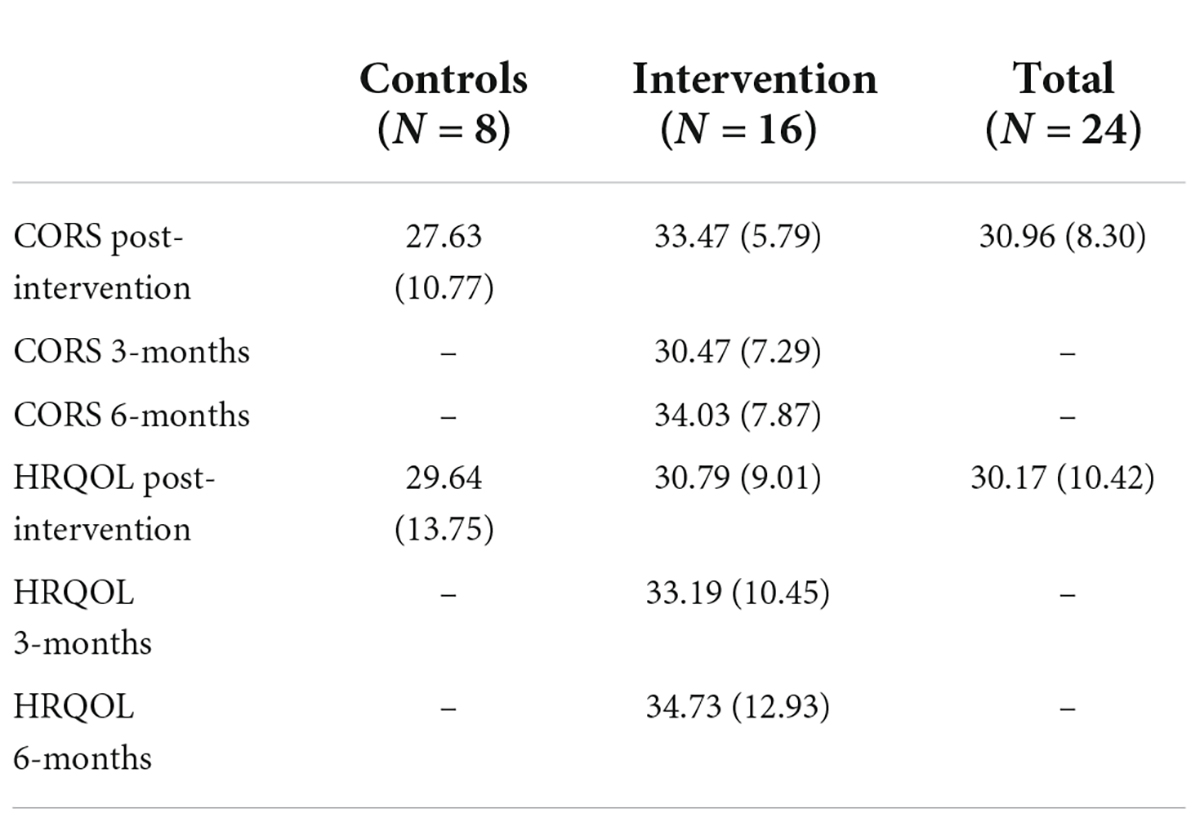
Table 3. Means and standard deviations (bracketed) for CORS and HRQOL post-intervention and at follow-up at 3-months and 6-months post-intervention, for total sample and separated by intervention group.
The DMP intervention group presented higher post-intervention scores than the control group for both CORS (i.e., 33.47 ± 5.79 vs. 27.63 ± 10.77) and HRQOL (i.e., 30.79 ± 9.01 vs. 29.64 ± 13.75). For those that took part in the DMP intervention mean scores for CORS showed lowest scores pre-intervention (mean = 25.93 ± 8.42), which increased post-intervention (mean = 33.47 ± 5.79; mean difference = 7.54) and further still at 6-months follow-up (mean = 34.03 ± 7.87), though this difference was fairly small (i.e., mean difference = 0.56) and was preceded by a drop in score at 3-months. In contrast HRQOL followed a continuous upward trajectory from post-intervention to 3-months and then 6-months follow-up for those that took part in the DMP intervention (see Table 3 for mean scores).
Strengths and difficulties questionnaire and sleep duration
Mean SDQ score was higher post-intervention (mean = 9.19 ± 5.49) than pre-intervention (mean = 7.88 ± 4.50) with a mean difference of 1.313 (SD = 3.04, 95%CI: –2.94, 0.31); this represents an improvement on this measure relating to teachers’ assessment of the child. Descriptive statistics indicate a higher mean number of minutes sleep post-intervention (mean = 485.00 ± 48.65) than pre-intervention (mean = 466.58 ± 59.59) with a mean difference of 18.42 min (SD = 43.68, 95%CI: –46.17, 9.34). This indicates that children slept approximately 18 min longer post-intervention than pre-intervention.
Child session rating scale
Figure 3 shows a bar chart presenting mean scores and error bars ratings across the eight DMP sessions. The figure shows that session quality was rated highly to begin with, specifically a mean of 8.47 (±0.73) was given for session 1, while sessions 2 and 3 received a mean score of 9.30 (±1.42) and 7.45 (±2.51) respectively. However, session quality dipped in the middle with a low of 3.51 (±2.72) for session 4 and ratings of 5.91 (±2.78), 5.36 (±2.99) and 5.03 (±2.89) for sessions 5, 6, and 7 respectively. However, session quality ratings increased in the last session with a mean score of 8.01 (±1.75), which is close to the session 1 ratings.
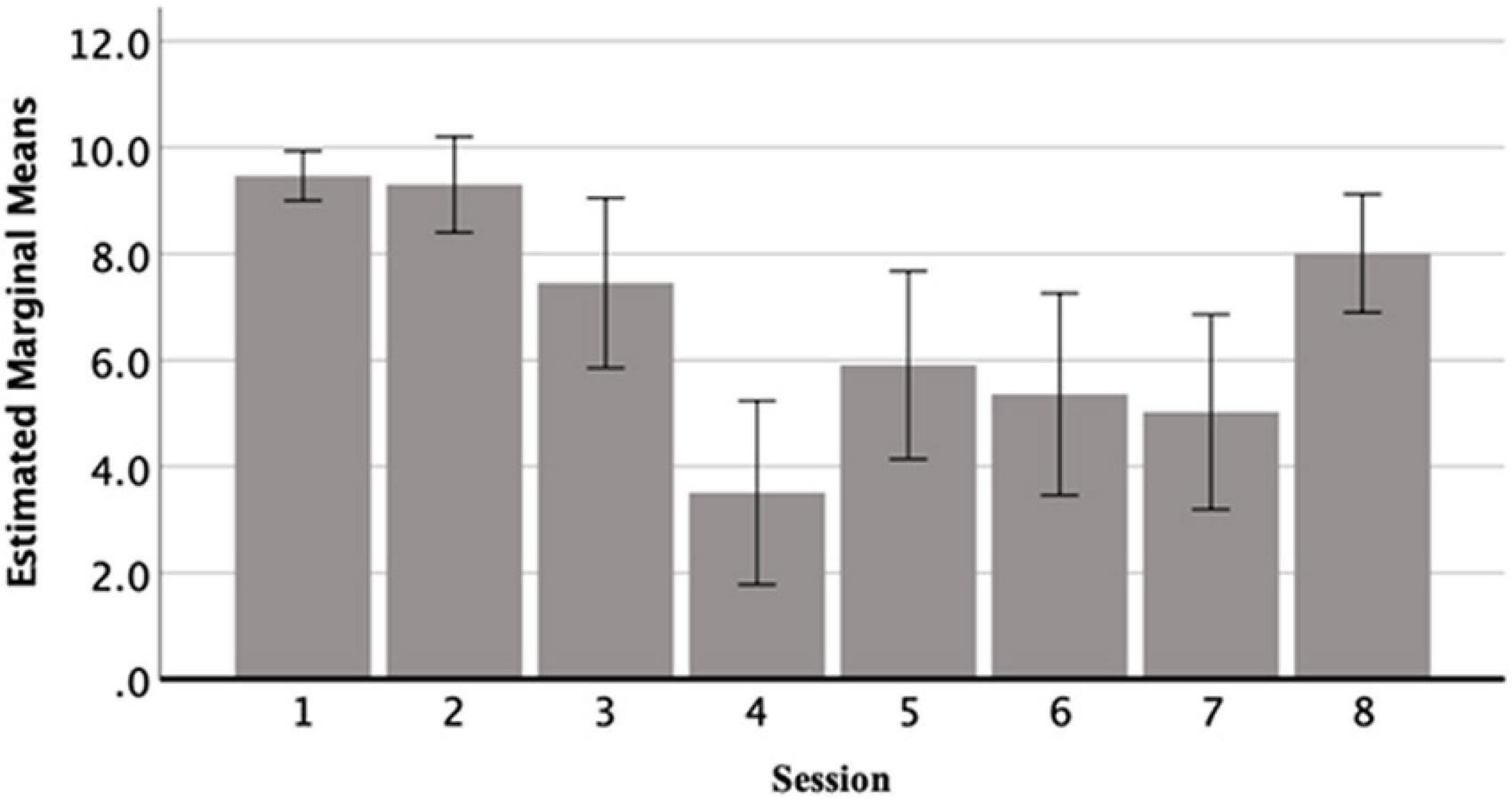
Figure 3. CSRS mean scores for each DMP session.
Adherence to therapeutic protocol
A rating was given for each of the 10 conditions by each rater for each group, yielding a total of 20 scores for the therapist (Rater A) and the researcher (Rater B). The Bland-Altman plot (Bland and Altman, 1986) evaluated the raters’ agreement. The mean score for raters A and B, for each of the 20 measurement points was calculated (A + B/2) along with the difference between rater scores (A - B). An overall disagreement of ±2 units or less was considered to be within the acceptable limits of agreement. The average of differences (d̄) between raters was –1.75, which was considered to be acceptable. This indicates that, on average, rater B (researcher) gave a rating of 1.75 units higher than rater A (therapist). The Bland-Altman plot (Figure 4) represents the difference between raters (A - B) against the mean of the two raters. The bias was –1.75 units, which is represented by the gap between the x-axis at 0 corresponding to zero differences, and the parallel line to the x-axis at –1.75 units.
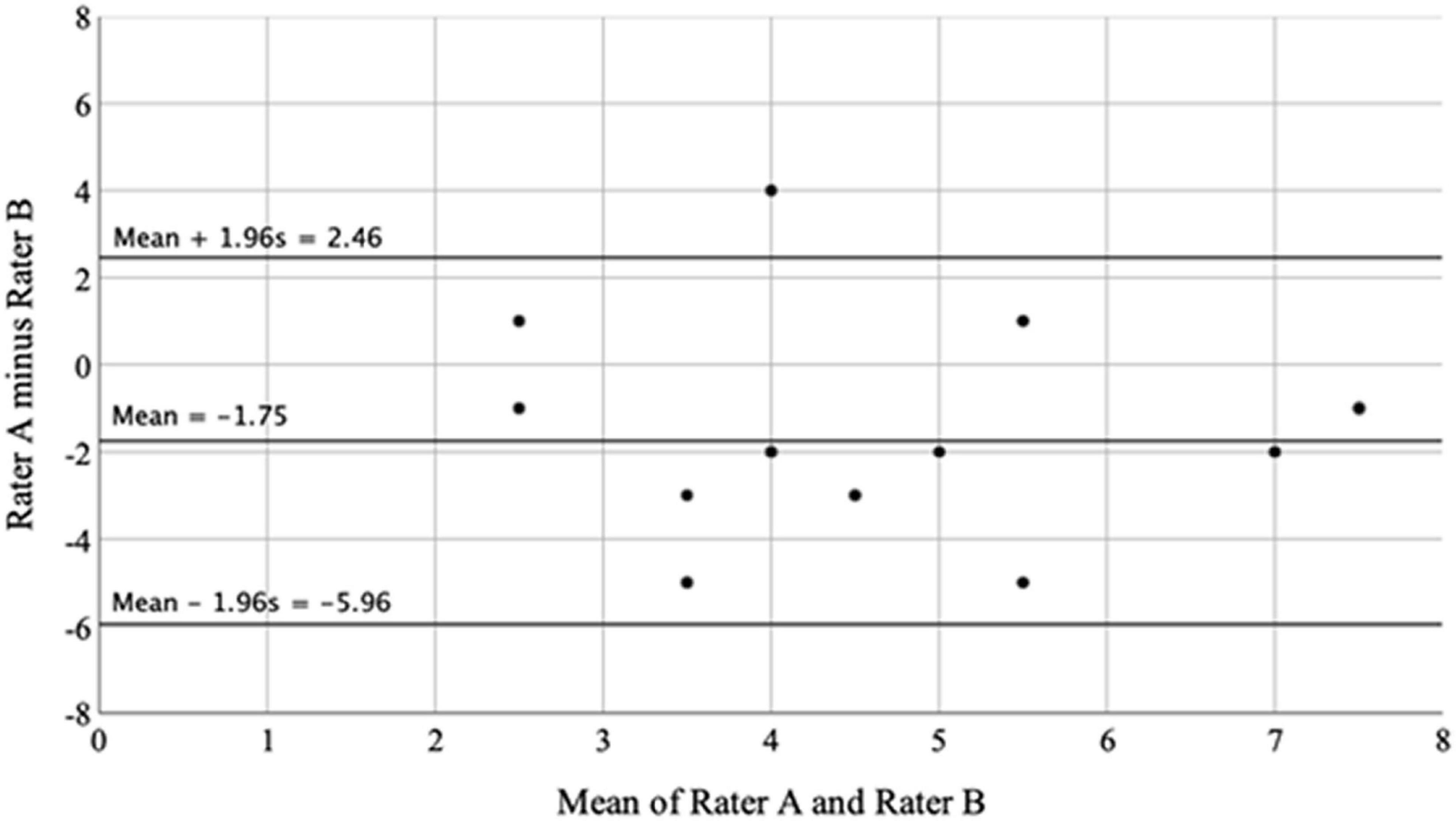
Figure 4. Bland-altman plot showing the difference between raters plotted against the mean of the two raters.
There did not appear to be any systematic bias, with no clear concentrations of data within, above or below this gap. The lack of agreement was summarized by calculating the bias estimated by the mean differences (d̄) and the standard deviation. We expected most of the differences to lie within d̄-1.96s and d̄ + 1.96s if the differences were normally distributed (Gaussian). In this study, s = 2.15, so that 95% of differences were within –5.96 and 2.46. These figures represented the lower and upper limits of agreement respectively. This showed that ratings made by rater A may be –5.96 units below or 2.46 units above rater B. It is important to note that the Bland-Altman plot did not indicate whether the agreement was sufficient or suitable to use one rater or the other indifferently. It also did not quantify the bias and the range of agreement within which 95% of the differences between one measurement and the other were included (Giavarina, 2015).
A one-sample t-test was used to determine whether the mean of difference between raters differed significantly from 0, with 0 representing no difference. A significant result indicated the presence of a fixed bias. Results from the one-sample t-test were significant (t19 = –3.642, P = 0.002, mean difference = –1.75, 95% CI: –2.76, –0.74). This indicated that rater A (therapist) was systematically rating less the adherence than rater B (researcher), with an average of 1.75 units less than rater B. This suggested that, if the therapist was considered the ideal candidate (or “gold standard”) in determining adherence to the therapeutic protocol, the researcher would not be an adequate substitute.
Discussion
Overall, the study design was followed as planned, however, some challenges which were encountered need to be considered in future studies. The main recruitment challenge in the DMP intervention was the term “dance.” Boys were reluctant to participate because of gender stereotypes and negative associations between men and dance. Replacing the term DMP with “movement therapy” made the recruitment easier. Another challenge was the provision of a safe therapeutic environment. The rooms were exposed to loud noises and interruptions, a challenge commonly faced in school-based psychotherapies (Danieli et al., 2019). The presence of an external observer, which was required from the first school for safeguarding purposes, interfered with children’s sense of safety and made children reluctant to share openly. It became necessary to seek an alternative school for the purposes of allowing for the DMP intervention to take place according to the protocol.
During the interviews post-intervention, children expressed improvements in their sense of wellbeing, creativity, and resourcefulness. They also discovered the multisensory potential of objects, such as in parachutes, fabrics, scarfs and other soft materials. This links back to the literature regarding creativity and imagination as one of the essential therapeutic elements (Karkou and Sanderson, 2006) that enables: access to difficult unconscious materials (Case and Dalley, 1992); safe self-expression (Lee, 2015); pleasure from artistic engagement (Csikszentmihalyi, 2002); and increased sense of empowerment (Zimmerman, 2000).
Children expressed that they felt more “confident” and “special.” Some children noted that they learned who is their “true self” and they felt less afraid to show this “true self” to others. Therefore, empowerment came alongside self-acceptance; both of which are key therapeutic ingredients (Sutherland et al., 2010; Sassen, 2012). Though self-acceptance, the acceptance of others also grew as children mentioned that they were trying more to understand others, rather than judging or blaming them. This might indicate that children developed ownership over their own behaviors and actions, and increased sense of self-control; both of which are key elements of the empowerment theory (Zimmerman, 2000).
Overall, the structure of the sessions remained consistent to the therapeutic protocol and no major modifications were recorded. Children’s ratings of session quality were higher for those sessions they said included enjoyable and entertaining activities. Children also rated higher the sessions with highly structured activities, indicating that they might prefer sessions which are well-structured and to some extent directive. These findings underline the value of triangulating the sources of information and the need to include children’s voice in research.
There were significant differences in the adherence ratings between the researcher (ZM) and the DMP (SB). It is possible that the DMP practitioner was more self-critical and reluctant to rate her own sessions too high. Vice versa, the researcher was more likely to rate the sessions higher due to confirmation bias: the researcher’s tendency to look for information or patterns in data that confirm their hypotheses, consciously or unconsciously. Nevertheless, the ratings helped to understand which therapeutic principles were achieved or were more difficult to be achieved. Finding balance between verbal and non-verbal communication was the most challenging therapeutic principle. This was because some children were very talkative, allowing less or no space for non-verbal communication, while other children were quiet, shy, and had limited verbal interactions with the group. Revisiting past experiences with direct impact on the here and now was also challenging for the sessions where conflicts and tension arose. It is likely that the therapeutic environment lacked the appropriate safety to openly revisit past experiences and it highlights the importance of establishing safety prior to opening up and sharing with the group. Working with empathy and warmth was the only principle that was met in all sessions.
Outcome measures: Child outcome rating scale, health related quality of life, strengths and difficulties questionnaire, and sleep duration
DMP had a positive effect on CORS, which were higher post-intervention for those that took part in the DMP intervention than the control group. The same was not true for HRQOL where post-intervention HRQOL scores were very similar between intervention and control groups. Previous research has found that DMP can significantly improve the quality of life of children and young people (i.e., Karkou et al., 2010; Madden et al., 2010; Abdulah and Abdulla, 2018). Moderate effects have been also found in DMP systematic reviews (Bradt et al., 2015), and meta-analyses (Koch et al., 2014, 2019). However, these reviews included children as well as young people and adults. Since there is no systematic review looking at the effectiveness of DMP for children’s quality of life, the existing evidence remains inconclusive.
According to the teachers’ questionnaires (SDQ), children presented fewer emotional and behavioral difficulties following the DMP intervention. These findings echo the results from previous research (Karkou et al., 2010; Abdulazeem, 2014; Alotaibi, 2017), which concluded that teachers noticed significant reduction in children’s emotional, conduct, hyperactivity, and peer relationships difficulties, as well as improvements in prosocial behavior.
Improvements in duration of sleep was also found through biomarkers (FitBits) with children sleeping approximately 18 min longer post-intervention than pre-intervention in the DMP group. These results were important considering the impact of sleep health on physical and psychological wellbeing. Particularly, sleep is a major influential factor of neurologic function that helps to maintain wellness, increase resilience (Raven et al., 2018), and even change perceptions of pain (Mondanaro et al., 2017). This is because neurologically, the mind remains active during sleep, unconsciously processing thoughts that have been put aside or dismissed (Feld and Born, 2017). Current evidence suggests that creative psychotherapies can soothe and sedate (Loewy, 2020), increasing comfort and decreasing anxiety impeding sleep capacity (Lund et al., 2020). Although this is the first study to explore changes in children’s sleep, preliminary evidence shows that creative psychotherapies improve sleep quality in adults (Wang et al., 2014; Kavurmaci et al., 2019) as well as in infants and toddlers (Loewy, 2020); while evidence comes primarily from music therapy.
This study found that both HRQOL and CORS improvements remained reasonably stable at the 6-month follow-up, indicating that DMP had a long-lasting impact for up to 6 months post-intervention. The systematic review that informed this pilot (Moula et al., 2020a) showed that only one out of the six included studies explored the long-term outcomes of school-based creative psychotherapies. The lack of follow-up or short follow-up may underestimate the benefits and fail to detect hazards, both of which can take longer to emerge (Llewellyn-Bennett et al., 2016). Therefore, long-term follow-up is highly recommended in future research to ascertain the strength of DMP over an extended period and the long-term impact of change on children’s life.
Limitations and future directions
Due to randomization, some children who did not get along with each other, were placed in the same group. Difficult dynamics in the group resulted in them hesitating to share personal experiences and feelings. If this study was to be replicated in the future, alternative methods of randomization would be recommended, such as cluster randomization. This could reduce the risk of harm that comes with mixing children who do not get along with each other and would enable the group to have more productive intervention. This could also result in closer adherence to the therapeutic protocol, making the intervention more replicable in future studies. Meeting each child separately before their allocation into groups would be highly recommended to understand whether they need one-to-one or group support and whether they can handle sharing the therapist’s attention. Offering a workshop to the school staff at the beginning would also be beneficial to secure understanding of the study, the intervention, and appropriate referrals.
The above suggestions, however, have direct implications on the cost of the study and, long term, the intervention itself. If this strategy was to be implemented, its cost-effectiveness should also be considered. Future studies that calculate the cost-effectiveness of the intervention are urgently needed to establish whether interventions such as this can offer emotional support to children in ways in which not only add value to the school environment but also offer a cost-effective solution to the development of long-term and/or more serious mental health problems.
It is suggested that future research should explore randomization strategies to overcome factors that hinder the therapeutic process, such as mixing children who do not get along well with each other. Cluster randomization or meeting each child one their own prior to allocation into groups could be beneficial strategies in future large-scale studies. If these strategies are employed, cost-effectiveness assessment should also be incorporated.
As this was a sub-study of a pilot, the aim was not to provide evidence that the proposed intervention is demonstrating a statistically significant improvement in our outcome measures, rather it is to test the study design (e.g., recruitment, randomization, follow-up) in terms of its implementation and chosen outcome measures to inform a future large-scale RCT design. Therefore, the focus is on presenting only descriptive statistics from the key outcome measures.
However, since this intervention was delivered to groups of children, rather than individual children, efforts to scale-up this or similar interventions should account for the methodological issues stemming from this study design, known also as Individually Randomized Group Treatment Trial (Pals et al., 2008). More specifically, it is important to consider that the participants in these groups share a similar history (e.g., attending the same school, in the same geographical location), share the treatment environment and interact with each other. As such, intraclass correlation can develop over time in group interventions, violating the major assumption of independence underlying the principal statistical methods used in RCTs (Pals et al., 2008). For this reason, expected intraclass correlations (ICCs) should be taken into account in future sample size estimations. This is expected to increase the required sample size given that the between-group heterogeneity and degrees of freedom should be based on the number of groups rather than the number of group members (Hoover, 2002). However, this method would ensure that the significance of the findings is not overestimated.
Furthermore, as the DMP intervention lasted approximately three months and the researcher (ZM) co-facilitated all sessions, the relationship between the children and the researcher evolved over time. It is therefore possible that children gave higher ratings in the questionnaires because of the close relationship with the researcher. The researcher’s dual role should be taken into account in the appraisal of the findings and in future similar interventions.
As this is a sub-study of a larger pilot randomized controlled study, our findings are limited to sixteen children from four classes and two schools within similar geographical locations. Considering the highly contextualized nature of childhood, the impact on children within different contexts may be different. Therefore, the findings need to be considered in combination with previous studies, such as those summarized in the literature review and discussion section.
Conclusion
The current study highlights the importance of using a mixed-methods approach to better understand the utility of creative arts-based interventions targeting mental health and wellbeing in mainstream schools. Utilizing both qualitative reports and quantitative measures the current study was able to demonstrate the viability of the DMP protocol and sensitivity of key outcome measures in a school-based setting. Moreover, the current study shows promising findings on the use of a DMP intervention in children in mainstream schools. Improvements were found for children’s wellbeing, life functioning, and sleep duration, as well as emotional and behavioral difficulties assessed by their teachers. Improvements in measures of wellbeing and quality of life were maintained at follow-up, until 6-months post-intervention. Although quality of life has been used extensively in public health research, it is not recommended to be used as a stand-alone measure due to its lack of sensitivity and specificity. In future interventions, widening the targeted outcomes is recommended to capture the impact more precisely. Within the qualitative reports, children expressed that they experienced positive outcomes, such as: self-expression; emotional regulation; mastery and acceptance of emotions; improved self-confidence, self-esteem, and self-worth; reduced stress; and development of positive relationships. Within the session ratings, children rated higher the sessions with entertaining activities and structured activities, indicating that they might prefer sessions which are well-structured and, to some extent, directive. These findings underline the value of collecting information from various sources, including children’s voice in research, while the involvement of children in the development of future outcome measures is also highly recommended. Overall, the study showed the effectiveness of the DMP intervention on children’s wellbeing and duration of sleep, however, several limitations to the study design are highlighted along with proposals for future studies, in particular with regards to randomization, statistical analysis and inclusion of outcome measures.
Data availability statement
The original contributions presented in this study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
Ethics statement
The studies involving human participants were reviewed and approved by Edge Hill University, Faculty of Health, Social Care, and Medicine. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Author contributions
ZM: conceptualization, methodology, investigation, analysis, writing—original draft, and visualization. JP: conceptualization, methodology, analysis, writing—review and editing, supervision, and visualization. SB: design and delivery of intervention and writing—review and editing. VK: conceptualization, methodology, writing—review and editing, and supervision. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2022.883334/full#supplementary-material
References
Abdulah, D. M., and Abdulla, B. M. O. (2018). Effectiveness of group art therapy on quality of life in paediatric patients with cancer: A randomized controlled trial. Comp. Ther. Med. 41, 180–185. doi: 10.1016/j.ctim.2018.09.020
Abdulazeem, A. (2014). Study of the impact of a movement therapy programme on perceptual-motor abilities and emotional wellbeing for children with mild learning difficulties in primary schools in Saudi Arabia. [Ph.D Thesis] Edinburgh:Queen Margaret University.
Aithal, A., Moula, Z., Karkou, V., Karaminis, T., Powell, J., and Makris, S. (2021). A systematic review of the contribution of dance movement psychotherapy towards the wellbeing of children with autism spectrum disorder. Front. Psychol. 12:719673. doi: 10.3389/fpsyg.2021.719673
Alotaibi, A., Karkou, V., Van Der Linden, M., and Irvine, L. (2017). “Movement therapy programme with children with mild learning difficulties in primary schools in Saudi Arabia: Links between motion and emotion,” in The oxford handbook of dance and wellbeing, eds V. Karkou, S. Oliver, and S. Lycouris (Oxford: Oxford University Press), 479–492.
Anderson, A. N., Kennedy, H., DeWitt, P., Anderson, E., and Wamboldt, M. Z. (2014). Dance/movement therapy impacts mood states of adolescents in a psychiatric hospital. Arts Psychother. 41, 257–262. doi: 10.1016/j.aip.2014.04.002
Asan, O., and Montague, E. (2014). Using video-based observation research methods in primary care health encounters to evaluate complex interactions. Inform. Primary Care 21, 161–170. doi: 10.14236/jhi.v21i4.72
Association for Dance Movement Psychotherapy [ADMPUK] (2013). What is Dance Movement Psychotherapy?.Bath, Eng:ADMPUK.
Atkinson, P., Coffey, A., and Delamont, S. (2003). Key Themes in Qualitative Research: Continuities and Changes. New York, NY: AltaMira Press.
Ballard, K. L., Sander, M. A., and Klimes-Dougan, B. (2014). School-related and social-emotional outcomes of providing mental health services in schools. J. Community Ment. Health 50, 145–149. doi: 10.1007/s10597-013-9670-y
Bareka, T., Panhofer, H., and Cigaran, S. R. (2019). Refugee children and body politics: The embodied political self and dance movement therapy. Body Mov. Dance Psychother. 14, 80–94. doi: 10.1080/17432979.2019.1614668
Berger, M. R. (1972). Bodily experience and expression of emotion. Monogr. Am. Dance Ther. Assoc. 2, 191–230.
Bland, J. M., and Altman, D. G. (1986). Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 327, 307–310. doi: 10.1016/S0140-6736(86)90837-8
Bradt, J., Shim, M., and Goodill, S. W. (2015). Dance/movement therapy for improving psychological and physical outcomes in cancer patients. Cochrane Database Syst. Rev. 1:CD007103. doi: 10.1002/14651858.CD007103.pub3
Braun, V., and Clarke, V. (2006). Using thematic analysis in psychology. Qual. Res. Psychol. 3, 77–101. doi: 10.1191/1478088706qp063oa
Brierley, J. A. (2017). The role of a pragmatist paradigm when adopting mixed methods in behavioural accounting research. Int. J. Behav. Account. Finance 6, 140–154. doi: 10.1504/IJBAF.2017.10007499
Bringhurst, D. L., Watson, C. W., Miller, S. D., and Duncan, B. L. (2006). The reliability and validity of the Outcome Rating Scale: A replication study of a brief clinical measure. J. Brief Ther. 5, 23–30.
Brooks, R., te Riele, K., and Maguire, M. (2017). Ethics and Education Research: Research Methods in Education Series. London: SAGE Publications.
Caan, W., Cassidy, J., Coverdale, G., Ha, M. A., Nicholson, W., and Rao, M. (2014). The value of using schools as community assets for health. Public Health 129, 3–16. doi: 10.1016/j.puhe.2014.10.006
Campbell, A., and Hemsley, S. (2009). Outcome Rating Scale and Session Rating Scale in psychological practice: Clinical utility of ultra-brief measures. Clin. Psychol. 12, 1–9. doi: 10.1080/13284200802676391
Capp, C. (2015). Our community, our schools: A case study of program design for school-based mental health services. Child. Schools 37, 241–248. doi: 10.1093/cs/cdv030
Chaiklin, S., and Schmais, C. (1986). “The chace approach to dance therapy,” in Eight theoretical approaches in dance/movement therapy, ed. P. L. Bernstein (Dubuque, IA: Kendall/Hunt Publishing Co).
Children’s Commissioner. (2021). The State of Children’s Mental Health Services 2020/21. https://www.bl.uk/collection-items/the-state-of-childrens-mental-health-services-202021(childrenscommissioner.gov.uk).
Children’s Commissioner for England (2017). Annual Report and Accounts. England:Children’s Commissioner for England
Creswell, J. W., and Plano Clark, V. L. (2017). Designing and Conducting Mixed Methods Research, 3rd Edn. London: Sage Publications.
Creswell, J. W. (2014). A concise introduction to mixed methods research. Thousand Oaks, CA: SAGE Publications.
Csikszentmihalyi, M. (2002). Flow-the Psychology of Happiness: The Classic Work on How to Achieve Happiness, London:Rider Publications.
Danieli, Y., Snir, S., Regev, D., and Adoni-Kroyanker, M. (2019). Suitability of the art therapy room and changes in outcome measures in the education system. Int. J. Art Ther. 24, 68–75. doi: 10.1080/17454832.2018.1564778
Dieterich-Hartwell, R., Goodill, S., and Koch, S. (2020). Dance/movement therapy with resettled refugees: A guideline and framework based on empirical data. Arts Psychother. 69:101664. doi: 10.1016/j.aip.2020.101664
Eke, L., and Gent, A. M. (2010). Working with withdrawn adolescents as a moving experience: A community resourced project exploring the usefulness of group dance movement psychotherapy within a school setting. Body Mov. Dance Psychother. 5, 45–57. doi: 10.1080/17432970903326953
Erfer, T., and Ziv, A. (2006). Moving toward cohesion: Group dance/movement therapy with children in psychiatry. Arts Psychother. 33, 238–246. doi: 10.1016/j.aip.2006.01.001
Feld, G. B., and Born, J. (2017). Sculpting memory during sleep: Concurrent consolidation and forgetting. Curr. Opin. Neurobiol. 44, 20–27. doi: 10.1016/j.conb.2017.02.012
Frizzell, C. (2006). The most accurate/updated reference is: Frizell, C. (2014) Discovering the language of the ecological body. Self Soc. 41, 15–21.
Goldie, I., Elliott, I., Regan, M., Bernal, L., and Makurah, L. (2016). Mental Health and Prevention: Taking Local Action. London: Mental Health Foundation.
Goodgame, J. (2007). Beyond words: Dance and movement sessions with young people with social, emotional and behavioural difficulties in Estonia. Support Learn. 22, 78–83. doi: 10.1111/j.1467-9604.2007.00451.x
Goodman, R. (2001). Psychometric properties of the strengths and difficulties questionnaire. J. Am. Acad. Child Adolesc. Psychiatry 40, 1337–1345. doi: 10.1097/00004583-200111000-00015
Grasser, L. R., Al-Saghir, H., Wanna, C., Spinei, J., and Javanbakht, A. (2019). Moving through the trauma: Dance/movement therapy as a somatic-based intervention for addressing trauma and stress among syrian refugee children. J. Am. Acad. Child Adolesc. Psychiatry 58, 1124–1126. doi: 10.1016/j.jaac.2019.07.007
Greenberg, M. T. (2010). School-based prevention: Current status and future challenges. Effect. Educ. 2, 27–52. doi: 10.1080/19415531003616862
Grönlund, E., Renck, B., and Weibull, J. (2005). Dance movement therapy as an alternative treatment for young boys diagnosed as ADHD: A pilot study. Am. J. Dance Ther. 27, 63–85. doi: 10.1007/s10465-005-9000-1
Higgins, J. P. T., and Green, S. (eds) (2011). Cochrane handbook for systematic reviews of interventions version 5.1.0. London:The Cochrane Collaboration.
Hoover, D. R. (2002). Clinical trials of behavioural interventions with heterogeneous teaching subgroup effects. Stat. Med. 21, 1351–1364. doi: 10.1002/sim.1139
Howe, K. R. (1988). Against the quantitative-qualitative incompatibility thesis or dogmas die hard. Educ. Res. 17, 10–16. doi: 10.3102/0013189X017008010
Jané-Llopis, E., and Braddick, F. (2008). Mental Health in Youth and Education: Consensus paper. Luxembourg: European Communities.
Jeong, Y. J., Hong, S. C., Lee, M. S., Park, M. C., Kim, Y. K., and Suh, C. M. (2005). Dance movement therapy improves emotional responses and modulates neurohormones in adolescents with mild depression. Int. J. Neurosci. 115, 1711–1720. doi: 10.1080/00207450590958574
Johnson, R. B., Onwuegbuzie, A. J., and Turner, L. A. (2007). Toward a definition of mixed methods research. J. Mixed Methods Res. 1, 112–133. doi: 10.1177/1558689806298224
Karkou, V. (2010). Arts therapies in schools: Research and practice. London: Jessica Kingsley Publishers.
Karkou, V., and Sanderson, P. (2006). Arts therapies: A research based map of the field. Edinburgh: Elsevier.
Karkou, V., Omylinska-Thurston, J., Parsons, A., Nair, K., Starkey, J., Haslam, S., et al. (2022). Bringing creative psychotherapies to primary nhs mental health services in the UK: A feasibility study on patient and staff experiences of arts for the blues workshops delivered at Improving Access To Psychological Therapies (IAPT) services. Couns. Psychother. Res. 22, 616–628. doi: 10.1002/capr.12544
Karkou, V., Fullarton, A., and Scarth, S. (2010). “Finding a way out of the labyrinth through Dance Movement Psychotherapy: Collaborative work in a mental health promotion programme in secondary schools,” in Arts Therapies in Schools: Research and Practice, ed. V. Karkou (London: Jessica Kingsley), 59–84.
Kavanagh, J., Oliver, S., Caird, J., Tucker, H., Greaves, A., Harden, A., et al. (2009). Inequalities and the Mental Health of Young People: A Systematic Review of Secondary School-Based Cognitive Behavioural Interventions. London: Institute of Education London.
Kavurmaci, M., Dayapoğlu, N., and Tan, M. (2019). Effect of music therapy on sleep quality. Alternat. Ther. Health Med. 1:AT5871.
Koch, S., Kunz, T., Lykou, S., and Cruz, R. (2014). Effects of dance movement therapy and dance on health-related psychological outcomes: A meta-analysis. Arts Psychother. 41, 46–64. doi: 10.1016/j.aip.2013.10.004
Koch, S. C., Riege, R., Tisborn, K., Biondo, J., Martin, L., and Beelmann, A. (2019). Effects of dance movement therapy and dance on health-related psychological outcomes: A meta-analysis update. Front. Psychol. 10:1806. doi: 10.3389/fpsyg.2019.01806
Koolaee, A., Sabzian, M., and Tagvaee, D. (2014). Moving toward integration: Group dance movement therapy with children in anger and anxiety. Middle East J. Nurs. 8, 3–7. doi: 10.5742/MEJN.2014.92586
Koshland, L., Wilson, J., and Wittaker, B. (2004). PEACE through dance/movement: Evaluating a violence prevention program. Am. J. Dance Ther. 26, 69–90. doi: 10.1007/s10465-004-0786-z
Lamond, I. (2010). Evaluating the impact of incorporating dance into the curriculum of children encountering profound and multiple learning difficulties. Body Mov. Dance Psychother. 5, 141–149. doi: 10.1080/17432970903315857
Lee, S. Y. (2015). Flow indicators in art therapy: Artistic engagement of immigrant children with acculturation gaps. art therapy. J. Am. Art Ther. Assoc. 32, 120–129. doi: 10.1080/07421656.2015.1060836
Llewellyn-Bennett, R., Bowman, L., and Bulbulia, R. (2016). Post-trial follow-up methodology in large randomized controlled trials: A systematic review protocol. Syst. Rev. 5:214. doi: 10.1186/s13643-016-0393-3
Loewy, J. (2020). Music therapy as a potential intervention for sleep improvement. Nat. Sci. Sleep 12, 1–9. doi: 10.2147/NSS.S194938
Low, D. C., Miller, S. D., and Squire, B. (2012). The Outcome Rating Scales (ORS) & Session Rating Scales (SRS): Feedback Informed Treatment in Child and Adolescent Mental Health Services (CAMHS). Cambridgeshire:Cambridgeshire andPeterborough NHS Trust.
Lund, H. N., Pedersen, I. N., Johnsen, S. P., et al. (2020). Music to improve sleep quality in adults with depression-related insomnia (MUSTAFI): Study protocol for a randomized controlled trial. Trials 21:305. doi: 10.1186/s13063-020-04247-9
Lundh, L. G., Wangby-Lundh, M., and Bjarehed, J. (2008). Self-reported emotional and behavioral problems in Swedish 14 to 15-year-old adolescents: A study with the self-report version of the Strengths and Difficulties Questionnaire. Scand. J. Psychol. 49, 523–532. doi: 10.1111/j.1467-9450.2008.00668.x
Madden, J. R., Mowry, P., Gao, D., Cullen, P. M., and Foreman, N. K. (2010). Creative arts therapy improves quality of life for pediatric brain tumor patients receiving outpatient chemotherapy. J. Pediatr. Oncol. Nurs. 27, 133–45. doi: 10.1177/1043454209355452
Meekums, B. (2008). Developing emotional literacy through individual Dance Movement Therapy: A pilot study. J. Emot. Behav. Diff. 13, 95–110. doi: 10.1080/13632750802027614
Miller, S. D., Duncan, B. L., Brown, J., Sparks, J., and Claud, D. (2003). The Outcome Rating Scale: A preliminary study of the reliability, validity, and feasibility of a brief visual analog measure. J. Brief Ther. 2, 91–100.
Mondanaro, J. F., Homel, P., Lonner, B., Shepp, J., Lichtensztein, M., and Loewy, J. V. (2017). Music therapy increases comfort and reduces pain in patients recovering from spine surgery. Am. J. Orthop. 46, E13–E22
Moula, Z. (2020). Child-Focused Process and Outcome Evaluation for Children in Primary Schools. [Ph.D Thesis] Ormskirk:Edge Hill University.
Moula, Z., Aithal, S., Karkou, V., and Powell, J. (2020a). A systematic review of child-focused outcomes and assessments of arts therapies delivered in primary mainstream schools. J. Child. Youth Serv. Rev. 112:104928. doi: 10.1016/j.childyouth.2020.104928
Moula, Z., Karkou, V., and Powell, J. (2019). A pilot randomised controlled trial of child-focused process and outcome evaluation of arts therapies at primary mainstream schools: Study protocol. Int. J. Arts Health 13, 173-188. doi: 10.1080/17533015.2019.1703198
Moula, Z., Powell, J., and Karkou, V. (2020b). An investigation of the effectiveness of arts therapies interventions on measures of quality of life and wellbeing: A pilot randomized controlled study in primary schools. Front. Psychol. 11:586134. doi: 10.3389/fpsyg.2020.586134
Muhs, N. (2021). Creating a Movement Group in the 2-Dimensional World: Using Dance/Movement Therapy Interventions to Build Connections for Children. [Ph.D Thesis]. Cambridge, MA:Lesley University.
Mullane, S., and Dunphy, K. (2017). “Dance movement therapy, student learning, and wellbeing in special education,” in The Oxford Handbook of Dance and Wellbeing, eds V. Karkou, S. Oliver, and S. Lycouris (Oxford: Oxford University Press), doi: 10.1093/oxfordhb/9780199949298.013.54
Muris, P., Meesters, C., and van den Berg, F. (2003). The Strengths and Difficulties Questionnaire (SDQ): Further evidence for its reliability and validity in a community sample of Dutch children and adolescents. Eur. Child Adolesc. Psychiatry 12, 1–8. doi: 10.1007/s00787-003-0298-2
Onwuegbuzie, A. J., and Johnson, R. B. (2006). The validity issue in mixed research. Res. Schools 13, 48–63.
Omylinska-Thurston, J., Karkou, V., Parsons, A., Nair, K., Dubrow-Marshall, L., Starkey, J., et al. (2020). Arts for the Blues: The development of a new evidence-based creative group psychotherapy for depression. Couns. Psychother. Res. 21, 597–607. doi: 10.1002/capr.12373
The World Health Organisation [WHO] (2004). Prevention of Mental Disorders: Effective Interventions and Policy Options. Nijmegen, MA: WHO Department of Mental Health and Substance Abuse.
Pals, S. L., Murray, D. M., Alfano, C. M., Shadish, W. R., Hannan, P. J., and Baker, W. L. (2008). Individually randomized group treatment trials: A critical appraisal of frequently used design and analytic approaches. Am. J. Public Health 98, 1418–1424. doi: 10.2105/AJPH.2007.127027
Patalay, P., Gondek, D., Moltrecht, B., Giese, L., Curtin, C., Stanković, M., et al. (2017). Mental health provision in schools: Approaches and interventions in 10 European countries. Glob. Ment. Health 4:E10. doi: 10.1017/gmh.2017.6
Raven, F., Van der Zee, E. A., Meerlo, P., and Havekes, R. (2018). The role of sleep in regulating structural plasticity and synaptic strength: Implications for memory and cognitive function. Sleep Med. Rev. 39, 3–11. doi: 10.1016/j.smrv.2017.05.002
Ravens-Sieberer, U., Wille, N., Badia, X., Bonsel, G., Burström, K., Cavrini, G., et al. (2010). Feasibility, reliability, and validity of the EQ-5D-Y: Results from a multinational study. Qual. Life Res. 19, 887–897. doi: 10.1007/s11136-010-9649-x
Redman, D. (2007). The Effectiveness of Dance/Movement Therapy as a Treatment for Students In a Public Alternative School Diagnosed with Attention Deficit Hyperactivity Disorder: a Pilot Study.[Ph.D Thesis] Philadelphia, PA: Drexel University.
Sassen, G. (2012). Drums and poems: An intervention promoting empathic connection and literacy in children. J. Creat. Ment. Health 7, 233–248. doi: 10.1080/15401383.2012.711712
Shuper-Engelhard, E. S., and Furlager, A. Y. (2021). Remaining held: Dance/movement therapy with children during lockdown. Body Mov. Dance Psychother. 16, 73–86. doi: 10.1080/17432979.2020.1850525
Snir, S., Hilbuch, A., Regev, D., and Orkibi, H. (2016). The role of art materials in the transferential relationship: Art psychotherapists’ perspective. Arts Psychother. 49, 19–26. doi: 10.1016/j.aip.2016.05.011
Stephan, S. H., Weist, M., Kataoka, S., Adelsheim, S., and Mills, C. (2007). Transformation of children’s mental health services: The role of school mental health. Psychiatr. Serv. 58, 1330–1338. doi: 10.1176/ps.2007.58.10.1330
Sutherland, J., Waldman, G., and Collins, C. (2010). Art therapy connection: Encouraging troubled youth to stay in school and succeed. J. Am. Art Ther. Assoc. 27, 69–74. doi: 10.1080/07421656.2010.10129720
Teddlie, C., and Tashakkori, A. (2009). Foundations of Mixed Methods Research: Integrating Quantitative and Qualitative: Approaches in the Social and Behavioral Sciences. London: Sage Publications.
Unkovich, G., Butté, C., and Butler, J. (2017). Dance Movement Psychotherapy with People with Learning Disabilities: Out of the Shadows, Into the Light. London: Routledge. doi: 10.4324/9781315183275
Wang, C. F., Sun, Y. L., and Zang, H. X. (2014). Music therapy improves sleep quality in acute and chronic sleep disorders: A meta-analysis of 10 randomized studies. Int. J. Nurs. Stud. 51, 51–62. doi: 10.1016/j.ijnurstu.2013.03.008
Weare, K., and Nind, M. (2011). Mental health promotion and problem prevention in schools: What does the evidence say? Health Promot. Int. 26, i29–i69. doi: 10.1093/heapro/dar075
Wille, N., Badia, X., Bonsel, G., Burström, K., Cavrini, G., Devlin, N., et al. (2010). Development of the EQ-5D-Y: A child-friendly version of the EQ-5D. Qual. Life Res. 19, 875–886. doi: 10.1007/s11136-010-9648-y
Yao, S., Zhang, C., Zhu, X., Jing, X., McWhinnie, C. M., and Abela, J. R. Z. (2009). Measuring adolescent psychopathology: Psychometric properties of the self-report Strengths and Difficulties Questionnaire in a sample of Chinese adolescents. J. Adolesc. Health 45, 55–62. doi: 10.1016/j.jadohealth.2008.11.006
Young Minds (2021). Coronavirus: Impact on Young People with Mental Health Needs. Available online at :https://www.bl.uk/collection-items/the-state-of-childrens-mental-health-services-202021(youngminds.org.uk). (accessed February 17, 2022).
Yvonne Feilzer, M. (2010). Doing mixed methods research pragmatically: Implications for the rediscovery of pragmatism as a research paradigm. J. Mixed Methods Res. 4, 6–16. doi: 10.1177/1558689809349691
Zimmerman, M. A. (2000). “Empowerment theory: Psychological, organizational, and community levels of analysis,” in Handbook of Community Psychology, eds J. Rappaport and E. Seidman (New York, NY: Springer Publications), 43–63. doi: 10.1007/978-1-4615-4193-6_2
Keywords: dance and movement, psychotherapy, children, schools, wellbeing, quality of life, sleep, randomized controlled study
Citation: Moula Z, Powell J, Brocklehurst S and Karkou V (2022) Feasibility, acceptability, and effectiveness of school-based dance movement psychotherapy for children with emotional and behavioral difficulties. Front. Psychol. 13:883334. doi: 10.3389/fpsyg.2022.883334
Received: 24 February 2022; Accepted: 21 July 2022;
Published: 22 August 2022.
Edited by:
Gian Mauro Manzoni, University of eCampus, ItalyReviewed by:
Einat Shuper Engelhard, University of Haifa, IsraelHanna Pohjola, University of Eastern Finland, Finland
Sandra Kay Lauffenburger, Independent Researcher, Canberra, ACT, Australia
Copyright © 2022 Moula, Powell, Brocklehurst and Karkou. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zoe Moula, z.moula@imperial.ac.uk