
A Social Return on Investment Evaluation of the Pilot Social Prescribing EmotionMind Dynamic Coaching Programme to Improve Mental Wellbeing and Self-Confidence

 , ,
, ,  ,
,
Abstract
:1. Introduction
1.1. Background
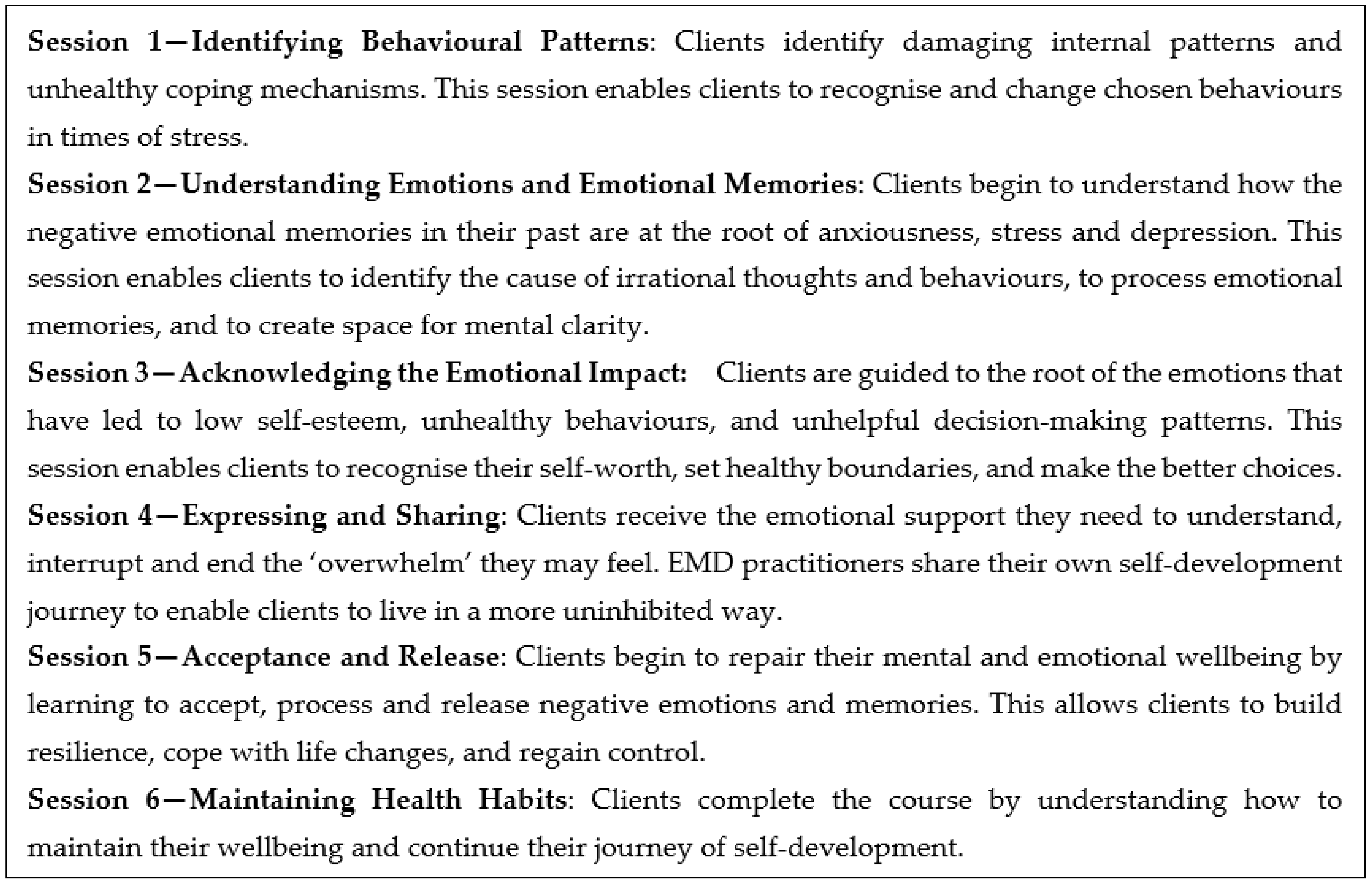
1.2. The EmotionMind Dynamic Programme
2. Materials and Methods
2.1. Social Return on Investment Methodology
- Identifying stakeholders;
- Developing a theory of change;
- Calculating inputs;
- Evidencing and valuing outcomes;
- Establishing impact;
- Calculating the SROI ratio.
2.2. Identifying Stakeholders
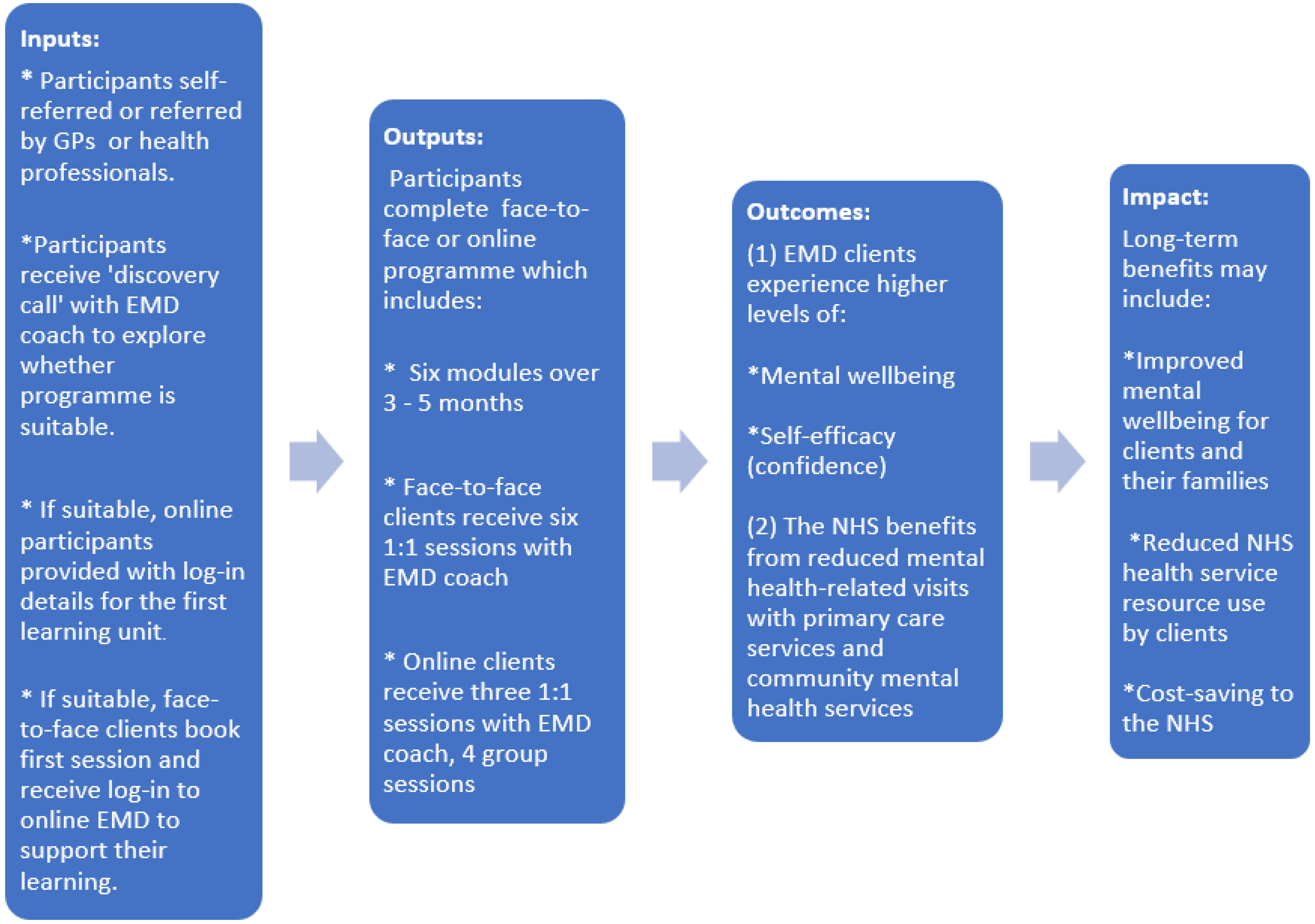
2.3. Theory of Change
2.4. Calculating Inputs
2.4.1. Product development costs
2.4.2. Consultancy costs
2.4.3. Website costs
2.4.4. Equipment and software costs
2.4.5. Overhead costs
2.4.6. Staff costs
2.5. Evidencing and Valuing Outcomes
2.5.1. Questionnaires
2.5.2. Client Service Receipt Inventory (CSRI)
2.5.3. Interviews
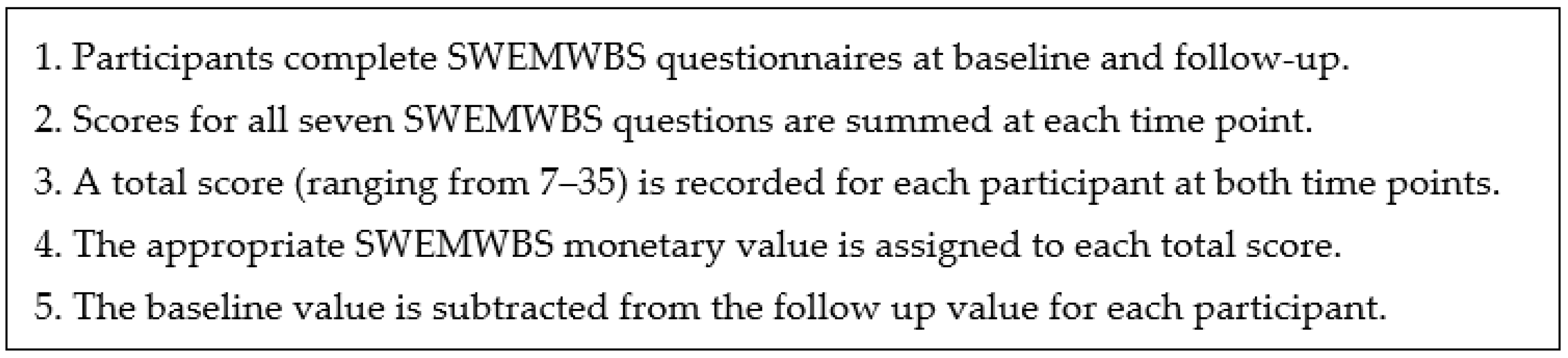
2.5.4. Wellbeing Valuation using the Social Value Calculator
2.5.5. Wellbeing Valuation using the Mental Health Social Value Calculator
2.6. Establishing Impact
2.7. Calculating the SROI Ratio
3. Results
3.1. Comparing Costs
3.2. Outcomes using the Social Value Calculator
3.3. Outcomes using the Mental Health Social Value Calculator
3.4. Outcomes from the CSRI Questionnaire
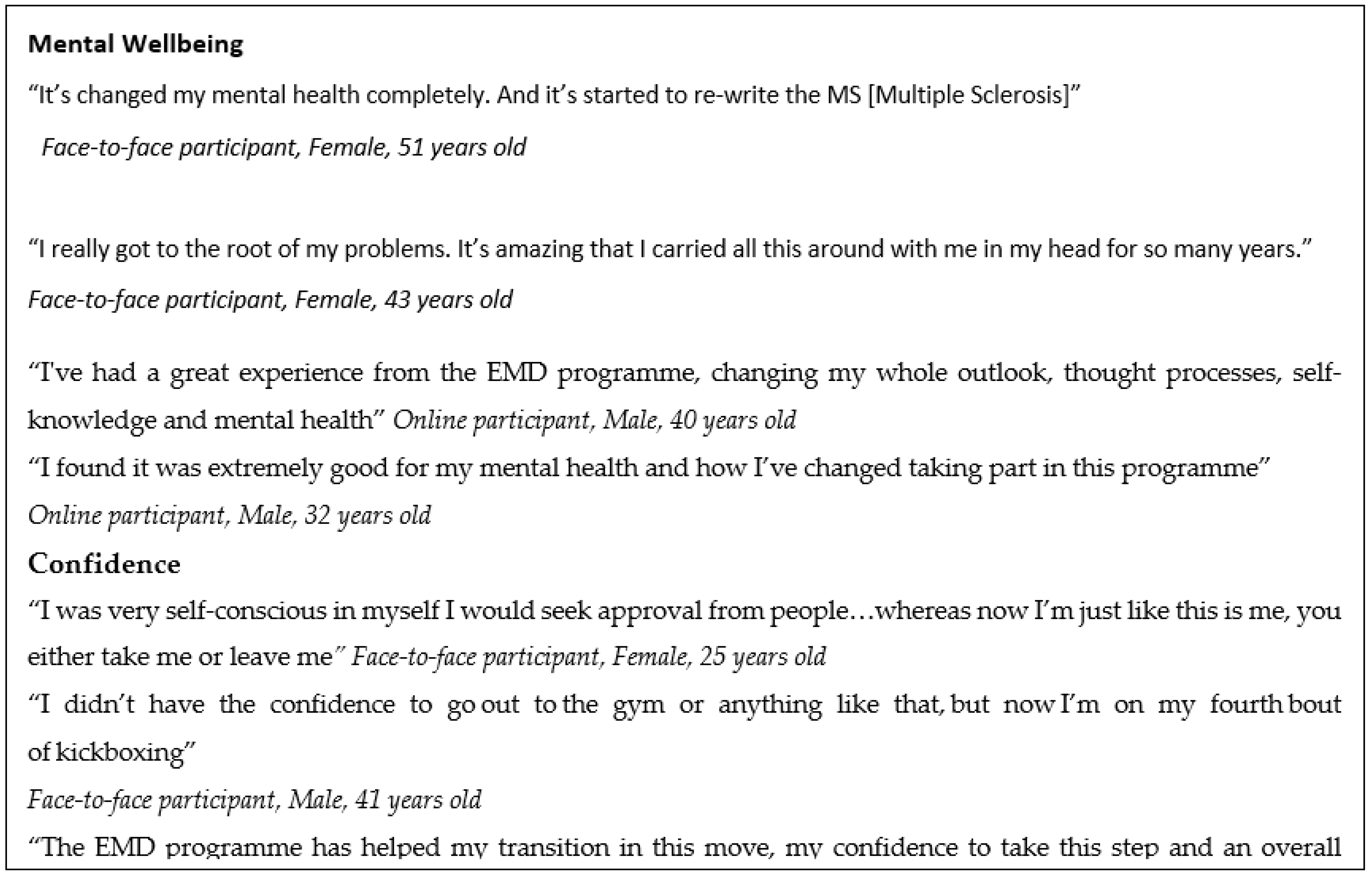
3.5. Outcomes (Non-Monetised) from Interviews
3.6. Calculating the SROI Ratio
4. Discussion
4.1. Strengths
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barrett, S.; Begg, S.; O’Halloran, P.; Kingsley, M. Cost-effectiveness of telephone coaching for physically inactive ambulatory care hospital patients: Economic evaluation alongside the Healthy4U randomised controlled trial. BMJ Open 2019, 9, e032500. [Google Scholar] [CrossRef] [PubMed]
- Bishop, L.; Hemingway, A.; Crabtree, S.A. Lifestyle coaching for mental health difficulties: Scoping review. J. Public Ment. Health 2018, 17, 29–44. [Google Scholar] [CrossRef]
- Bolsinger, J.; Jaeger, M.; Hoff, P.; Theodoridou, A. Challenges and Opportunities in Building and Maintaining a Good Therapeutic Relationship in Acute Psychiatric Settings: A Narrative Review. Front. Psychiatry 2020, 10, 965. [Google Scholar] [CrossRef]
- Brog, N.A.; Hegy, J.K.; Berger, T.; Znoj, H. An internet-based self-help intervention for people with psychological distress due to COVID-19: Study protocol for a randomized controlled trial. Trials 2021, 22, 171. [Google Scholar] [CrossRef] [PubMed]
- Chesney, E.; Goodwin, G.M.; Fazel, S. Risks of all-cause and suicide mortality in mental disorders: A meta-review. World Psychiatry 2014, 13, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Dancer, S. Additionality Guide, 4th ed.; Homes and Communities Agency: London, UK, 2014. [Google Scholar]
- Green, L.S.; Oades, L.G.; Grant, A.M. Cognitive-behavioral, solution-focused life coaching: Enhancing goal striving, well-being, and hope Cognitive-behavioral, solution-focused life coaching: Enhancing goal striving, well-being, and hope. J. Posit. Psychol. 2006, 1, 142–149. [Google Scholar] [CrossRef]
- Health and Social Care Committee. Clearing the Backlog Caused by the Pandemic Ninth Report of Session 2021–2022 Report, Together with Formal Minutes Relating to the Report. 2021. Available online: www.parliament.uk/hsccom (accessed on 19 May 2022).
- HM Treasury. The Green Book Central Government Guidance on Appraisal and Evaluation. 2022. Available online: www.gov.uk/official-documents (accessed on 17 May 2022).
- HSCIC, Health Survey for England. Mental Health Problems; HSCIC: London, UK, 2014. Available online: http://healthsurvey.hscic.gov.uk/support-guidance/public-health/health-survey-for-england-2014/key-findings.aspx (accessed on 25 August 2022).
- Ilyas, A.; Chesney, E.; Patel, R. Improving life expectancy in people with serious mental illness: Should we place more emphasis on primary prevention? Br. J. Psychiatry 2017, 211, 194. [Google Scholar] [CrossRef] [PubMed]
- Katsikis, D.; Kostogiannis, C.; Dryden, W. A Rational-Emotive Behavior Approach in Life Coaching. Journal of Evidence-Based Psychotherapies. 2016. Available online: https://psycnet.apa.org/record/2016-21529-002 (accessed on 28 April 2022).
- Lattie, E.G.; Adkins, E.C.; Winquist, N.; Stiles-Shields, C.; Wafford, Q.E.; Graham, A.K. Digital Mental Health Interventions for Depression, Anxiety, and Enhancement of Psychological Well-Being Among College Students: Systematic Review. J. Med. Internet Res. 2019, 21, e12869. [Google Scholar] [CrossRef] [PubMed]
- Leon, A.C.; Davis, L.L.; Kraemer, H.C. The Role and Interpretation of Pilot Studies in Clinical Research. J. Psychiatr. Res. 2011, 45, 626. [Google Scholar] [CrossRef] [PubMed]
- Jeannotte, A.M.; Hutchinson, D.M.; Kellerman, G. Time to Change for Mental Health and Well-being via Virtual Professional Coaching: Longitudinal Observational Study. J. Med. Internet Res. 2021, 23, e27774. [Google Scholar] [CrossRef] [PubMed]
- Mahase, E. NHS England sets out ambitious new mental health access standards to deal with pandemic demand. BMJ 2022, 376, o486. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. How NICE Measures Value for Money in Relation to Public Health Interventions; Local Government Briefing; National Institute for Health and Care Excellence: London, UK, 2013. [Google Scholar]
- Michaelson, J.; Mahony, S.; Schifferes, J. Measuring Well-Being: A Guide for Practitioners; New Economics Foundation: London, UK, 2012. [Google Scholar]
- NHS. The NHS Long Term Plan. 2019. Available online: www.longtermplan.nhs.uk (accessed on 7 April 2020).
- NHS England. Widespread Support for Proposed NHS Mental Health Access Standards for Patients. 2022. Available online: https://www.england.nhs.uk/2022/02/widespread-support-for-proposed-nhs-mental-health-access-standards-for-patients/ (accessed on 17 May 2022).
- Nicholls, J.; Lawlor, E.; Nietzert, E. A Guide to Social Return on Investment; The SROI Network: Liverpool, UK, 2012. [Google Scholar]
- Life Coach Hourly Pay in United Kingdom. 2021. Available online: https://www.payscale.com/research/UK/Job=Life_Coach/Salary (accessed on 25 January 2022).
- Life Coach Job Profile. 2022. Available online: https://www.prospects.ac.uk/job-profiles/life-coach (accessed on 13 June 2022).
- Raven, M. Analysis of Mortality in Mental Disorders. JAMA Psychiatry 2015, 72, 1150. [Google Scholar] [CrossRef] [PubMed]
- Rogers, C.R. Client-Centered Therapy: Its Current Practice, Implications and Theory; Constable & Robinson Ltd.: London, UK, 2003. [Google Scholar]
- Schwarzer, R.; Jerusalem, M.; Johnston, M. Generalized Self-Efficacy Scale; American Psychological Association: Worcester, MA, USA, 1995. [Google Scholar]
- Stats Wales. Welsh Index of Multiple Deprivation. 2019. Available online: https://statswales.gov.wales/Catalogue/Community-Safety-and-Social-Inclusion/Welsh-Index-of-Multiple-Deprivation (accessed on 24 May 2022).
- Stewart-Brown, S.; Tennant, A.; Tennant, R.; Platt, S.; Parkinson, J.; Weich, S. Internal construct validity of the Warwick-Edinburgh Mental Well-being Scale (WEMWBS): A Rasch analysis using data from the Scottish Health Education Population Survey. Health Qual. Life Outcomes 2009, 7, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.B.; Ruzek, J.I.; Fitzsimmons-Craft, E.E.; Sadeh-Sharvit, S.; Topooco, N.; Weissman, R.S.; Eisenberg, D.; Mohr, D.; Graham, A.; Jacobi, C.; et al. Using Digital Technology to Reduce the Prevalence of Mental Health Disorders in Populations: Time for a New Approach. J. Med. Internet Res. 2020, 22, e17493. [Google Scholar] [CrossRef] [PubMed]
- Trotter, L.; Rallings Adams, M.-K. Valuing Improvements in Mental Health: Applying the Wellbeing Valuation Method to WEMWBS. London, UK. 2017. Available online: www.understandingsociety.ac.uk (accessed on 7 December 2021).
- UK Government. Minimum Wage Rates for April 2021 to March 2022. 2022. Available online: https://www.gov.uk/government/publications/minimum-wage-rates-for-2022 (accessed on 31 March 2022).
- Vaingankar, J.A.; Abdin, E.; Chong, S.A.; Sambasivam, R.; Seow, E.; Jeyagurunathan, A.; Picco, L.; Stewart-Brown, S.; Subramaniam, M. Psychometric properties of the short Warwick Edinburgh mental well-being scale (SWEMWBS) in service users with schizophrenia, depression and anxiety spectrum disorders. Health Qual. Life Outcomes 2017, 15, 153. [Google Scholar] [CrossRef] [PubMed]
- Wilson, H.; Finch, D. Unemployment and Mental Health Why Both Require Action for Our COVID-19 Recovery; Health Foundation: London, UK, 2021. [Google Scholar]
- Wood, M.J.; Wilson, H.M.; Parry, S.L. Exploring the development and maintenance of therapeutic relationships through e-Health support: A narrative analysis of therapist experiences. J. Med. Access 2021, 5, 23992026211018087. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outcome | Outcome Measure | Wellbeing Valuation Method |
|---|---|---|
| Mental wellbeing | SWEMWBS | Mental health social value calculator v.1.0 |
| Self-efficacy | GSES | Social value calculator v.4.0 |
| Face-To-Face Clients | Online Clients | |
|---|---|---|
| Mean age | 43 years old | 44 years old |
| Gender | 73% female, 27% male | 65% female, 35% male |
| Ethnic origin | 100% White British | 100% White British |
| Main reason for enrolment | 67% enrolled citing depression | 47% enrolled citing depression |
| Weekly household income | GBP 325 | GBP 323 |
| Willingness to pay for EMD | GBP 730 | GBP 600 |
| Mean SWEMWBS score at baseline | 13 | 20 |
| Mean SWEMWBS score at follow-up | 28 | 26 |
| Mean GSES score at baseline | 16 | 26 |
| Mean GSES score at follow-up | 35 | 31 |
| Face-To-Face Clients | Online Clients | |
|---|---|---|
| Reported improvement of 1 point or more | 100% (15/15) | 88% (15/17) |
| Reported improvement of 5 points or more | 100% (15/15) | 65% (11/17) |
| Reported improvement of 10 points or more | 93% (14/15) | 29% (5/17) |
| Face-To-Face Clients | Online Clients | |
|---|---|---|
| Reported improvement of 1 point or more | 100% (15/15) | 82% (14/17) |
| Reported improvement of 5 points or more | 100% (15/15) | 59% (10/17) |
| Reported improvement of 10 points or more | 93% (14/15) | 18% (3/17) |
| Cost Category | Face-To-Face EMD Programme | Online EMD Programme |
|---|---|---|
Product development costs
| GBP 488 with 180-month amortisation GBP 458 with 180-month amortisation n/a GBP 30 with 180-month amortisation | GBP 677 with 180-month amortisation GBP 458 with 180-month amortisation GBP 189 with 180-month amortisation GBP 30 with 180-month amortisation |
Consultancy costs
| GBP 1179 with 180-month amortisation GBP 617 with 180-month amortisation GBP 33 with 180-month amortisation GBP 240 with 180-month amortisation GBP 289 with 180-month amortisation | GBP 1179 with 180-month amortisation GBP 617 with 180-month amortisation GBP 33 with 180-month amortisation GBP 240 with 180-month amortisation GBP 289 with 180-month amortisation |
Website costs
| GBP 5736 GBP 4080 GBP 256 GBP 1400 | GBP 5736 GBP 4080 GBP 256 GBP 1400 |
Equipment and software costs
| GBP 904 GBP 300 GBP 192 GBP 120 GBP 30 GBP 117 GBP 145 | GBP 904 GBP 300 GBP 192 GBP 120 GBP 30 GBP 117 GBP 145 |
Overhead costs
| GBP 1477 GBP 84 GBP 1158 GBP 235 | GBP 1477 GBP 84 GBP 1158 GBP 235 |
Staffing costs
| GBP 23,944 GBP 12,361 n/a n/a GBP 11,583 | GBP 14,330 GBP 2335 GBP 183 GBP 229 GBP 11,583 |
| Total annual cost with 180-month amortisation for start-up product development costs and consultancy costs | GBP 33,728 | GBP 24,303 |
| Total cost per client per year | GBP 2248 (n = 15) | GBP 1430 (n = 17) |
| Outcome: Confidence | Net Quantity | Financial Value (per Annum) | Total Social Value (per Annum) | Deadweight | Attribution | Displacement | Total Social Value (per Annum) | Social Value per Client |
|---|---|---|---|---|---|---|---|---|
| Face-to-face (n = 15) | 15/15 | GBP 13,080 | GBP 196,200 | 10% (×0.9) | 17% (×0.83) | 8% (×0.92) | GBP 134,836 | GBP 8989 |
| Online (n = 17) | 10/17 | GBP 13,080 | GBP 130,800 | 19% (×0.81) | 40% (×0.60) | 10% (×0.90) | GBP 57,212 | GBP 3365 |
| ID | Baseline (T1) | T1 Value | Follow-Up (T2) | T2 Value | Difference (T2-T1) | After Deadweight (27%) |
|---|---|---|---|---|---|---|
| 1 | 13 | 0 | 35 | GBP 26,793 | GBP 26,793 | GBP 19,559 |
| 2 | 11 | 0 | 33 | GBP 26,175 | GBP 26,175 | GBP 19,108 |
| 3 | 19 | GBP 17,561 | 33 | GBP 26,175 | GBP 8,614 | GBP 6288 |
| 4 | 7 | 0 | 35 | GBP 26,793 | GBP 26,793 | GBP 19,559 |
| 5 | 10 | 0 | 20 | GBP 17,561 | GBP 17,561 | GBP 12,820 |
| 6 | 14 | 0 | 31 | GBP 25,856 | GBP 25,856 | GBP 18,875 |
| 7 | 13 | 0 | 28 | GBP 24,877 | GBP 24,877 | GBP 18,160 |
| 8 | 12 | 0 | 29 | GBP 25,480 | GBP 25,480 | GBP 18,600 |
| 9 | 12 | 0 | 30 | GBP 25,480 | GBP 25,480 | GBP 18,600 |
| 10 | 9 | 0 | 24 | GBP 22,944 | GBP 22,944 | GBP 16,749 |
| 11 | 12 | 0 | 29 | GBP 25,480 | GBP 25,480 | GBP 18,600 |
| 12 | 8 | 0 | 27 | GBP 24,877 | GBP 24,877 | GBP 18,160 |
| 13 | 16 | GBP 9639 | 27 | GBP 24,877 | GBP 15,238 | GBP 11,124 |
| 14 | 17 | GBP 12,255 | 25 | GBP 24,225 | GBP 11,970 | GBP 8738 |
| 15 | 18 | GBP 12,255 | 29 | GBP 25,480 | GBP 13,225 | GBP 9654 |
| Total | GBP 51,710.00 | GBP 373,073.00 | GBP 321,363.00 | GBP 234,595 | ||
| Total social value per client (n = 15) | GBP 15,640 | |||||
| ID | Baseline (T1) | T1 Value | Follow-Up (T2) | T2 Value | Difference (T2-T1) | After Deadweight (27%) |
|---|---|---|---|---|---|---|
| 1 | 26 | GBP 24,225.00 | 29 | GBP 25,480.00 | GBP 1,255.00 | GBP 916 |
| 2 | 8 | GBP 0 | 22 | GBP 21,049.00 | GBP 21,049.00 | GBP 15,365 |
| 3 | 18 | GBP 12,255.00 | 15 | GBP 9,639.00 | −GBP 2616.00 | −GBP 1910 |
| 4 | 17 | GBP 12,255.00 | 28 | GBP 24,877.00 | GBP 12,622.00 | GBP 9214 |
| 5 | 21 | GBP 21,049.00 | 28 | GBP 24,877.00 | GBP 3828.00 | GBP 2794 |
| 6 | 20 | GBP 17,561.00 | 26 | GBP 24,225.00 | GBP 6664.00 | GBP 4865 |
| 7 | 21 | GBP 21,049.00 | 28 | GBP 24,877.00 | GBP 3828.00 | GBP 2794 |
| 8 | 13 | GBP 0 | 28 | GBP 24,877.00 | GBP 24,877.00 | GBP 18,160 |
| 9 | 18 | GBP 12,255.00 | 24 | GBP 22,944.00 | GBP 10,689.00 | GBP 7803 |
| 10 | 23 | GBP 22,944.00 | 34 | GBP 26,175.00 | GBP 3231.00 | GBP 2359 |
| 11 | 24 | GBP 22,944.00 | 26 | GBP 24,225.00 | GBP 1281.00 | GBP 935 |
| 12 | 22 | GBP 21,049.00 | 25 | GBP 24,225.00 | GBP 3176.00 | GBP 2318 |
| 13 | 21 | GBP 21,049.00 | 28 | GBP 24,877.00 | GBP 3828.00 | GBP 2794 |
| 14 | 28 | GBP 24,877.00 | 27 | GBP 24,877.00 | GBP 0 | GBP 0 |
| 15 | 18 | GBP 12,255.00 | 25 | GBP 24,225.00 | GBP 11,970.00 | GBP 8738 |
| 16 | 21 | GBP 21,049.00 | 22 | GBP 21,049.00 | GBP 0 | GBP 0 |
| 17 | 22 | GBP 21,049.00 | 34 | GBP 26,175.00 | GBP 5126.00 | GBP 3742 |
| Total | GBP 287,865.00 | GBP 398,673.00 | GBP 110,808.00 | GBP 80,890 | ||
| Total social value per client (n = 17) | GBP 4758 | |||||
| Type of client | 3 Months before Programme | 3 Months during Programme | Difference in Visits | Cost per Visit | Cost Saving per 3 Months | Cost Saving per 12 Months |
|---|---|---|---|---|---|---|
| Face-to-face clients (n = 15) | ||||||
| GP visits | 19 | 9 | 10 | GBP 39/visit 1 | GBP 390 | GBP 1,560 |
| Nurse | 2 | 0 | 2 | GBP 44/visit 1 | GBP 88 | GBP 352 |
| Psychologist | 9 | 0 | 9 | GBP 58/visit 1 | GBP 522 | GBP 2088 |
| Mental health nurse | 1 | 0 | 1 | GBP 21/visit 1 | GBP 21 | GBP 84 |
| Total cost saving | GBP 1021 | GBP 4084 | ||||
| Total cost saving per face-to-face client | GBP 272 | |||||
| Online clients (n = 17) | ||||||
| GP visits | 5 | 1 | 4 | GBP 39/visit 1 | GBP 156 | GBP 624 |
| Nurse | 1 | 1 | 0 | GBP 44/visit 1 | GBP 0 | GBP 0 |
| Psychologist | 1 | 1 | 0 | GBP 58/visit 1 | GBP 0 | GBP 0 |
| Mental health nurse | 1 | 3 | -2 | GBP 21/visit 1 | −GBP 42 | −GBP 168 |
| Total cost saving | GBP 114 | GBP 456 | ||||
| Total cost saving per online client | GBP 27 | |||||
| SROI Ratio (Social Value Calculator) | SROI Ratio (Mental Health Social Value Calculator) | |
|---|---|---|
| Total social value per face-to-face client | GBP 8989 | GBP 15,640 |
| NHS cost savings per face-to-face client | GBP 272 | GBP 272 |
| Total financial value per face-to-face client | GBP 9261 | GBP 15,912 |
| Total cost per face-to-face client | GBP 2248 | GBP 2248 |
| SROI ratio for face-to-face clients | GBP 4.12: GBP 1 | GBP 7.08: GBP 1 |
| Total social value per online client | GBP 3365 | GBP 4758 |
| NHS cost savings per online client | GBP 27 | GBP 27 |
| Total financial value per online client | GBP 3392 | GBP 4785 |
| Total cost per online client | GBP 1430 | GBP 1430 |
| SROI ratio for online clients | GBP 2.37: GBP 1 | GBP 3.35: GBP 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Makanjuola, A.; Lynch, M.; Hartfiel, N.; Cuthbert, A.; Wheeler, H.T.; Edwards, R.T. A Social Return on Investment Evaluation of the Pilot Social Prescribing EmotionMind Dynamic Coaching Programme to Improve Mental Wellbeing and Self-Confidence. Int. J. Environ. Res. Public Health 2022, 19, 10658. https://doi.org/10.3390/ijerph191710658
Makanjuola A, Lynch M, Hartfiel N, Cuthbert A, Wheeler HT, Edwards RT. A Social Return on Investment Evaluation of the Pilot Social Prescribing EmotionMind Dynamic Coaching Programme to Improve Mental Wellbeing and Self-Confidence. International Journal of Environmental Research and Public Health. 2022; 19(17):10658. https://doi.org/10.3390/ijerph191710658
Chicago/Turabian StyleMakanjuola, Abraham, Mary Lynch, Ned Hartfiel, Andrew Cuthbert, Hayley T. Wheeler, and Rhiannon Tudor Edwards. 2022. "A Social Return on Investment Evaluation of the Pilot Social Prescribing EmotionMind Dynamic Coaching Programme to Improve Mental Wellbeing and Self-Confidence" International Journal of Environmental Research and Public Health 19, no. 17: 10658. https://doi.org/10.3390/ijerph191710658