

The Required Competencies of Bachelor- and Master-Educated Nurses in Facilitating the Development of an Effective Workplace Culture in Nursing Homes: An Integrative Review
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Search Method
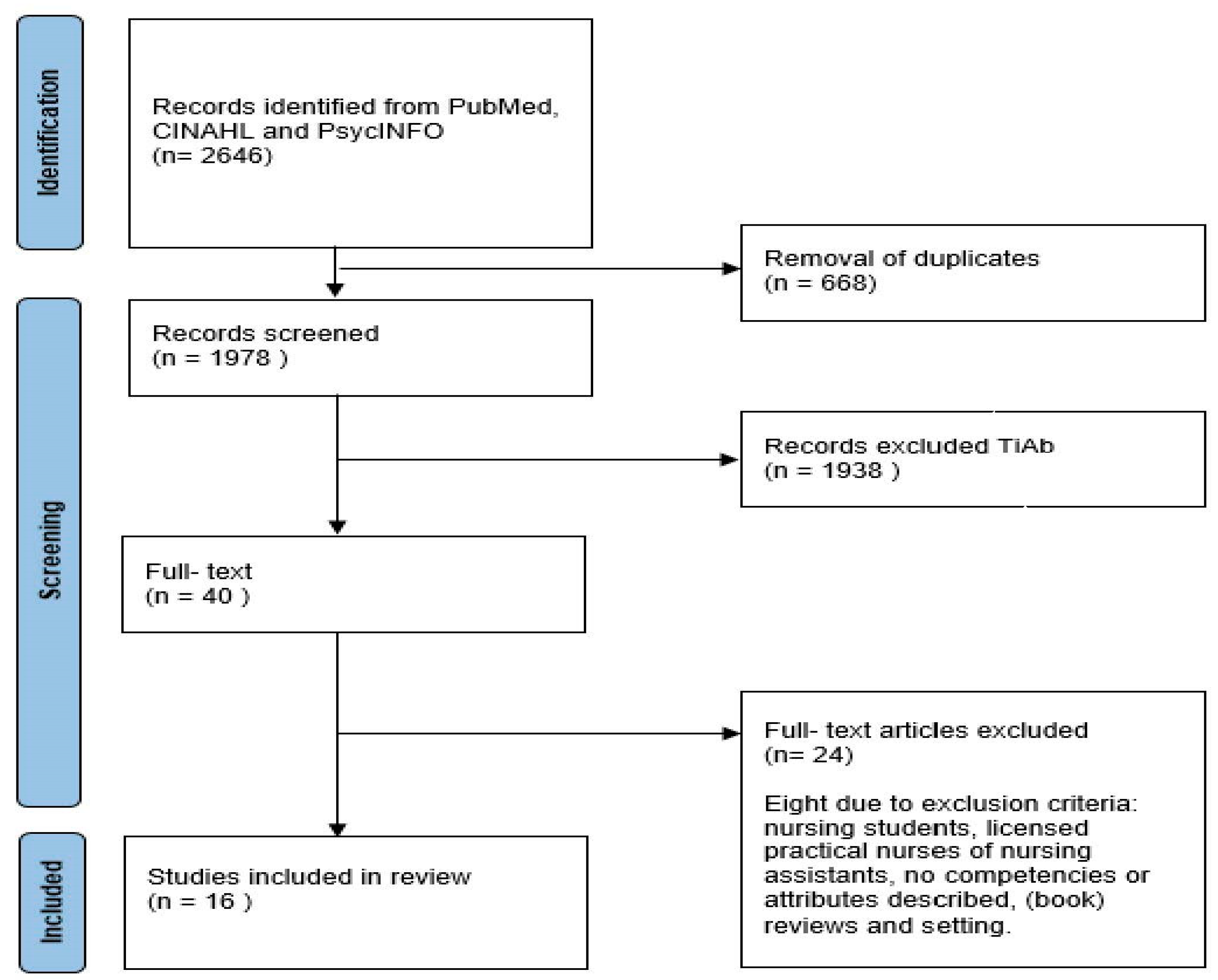
2.3. Search Outcome
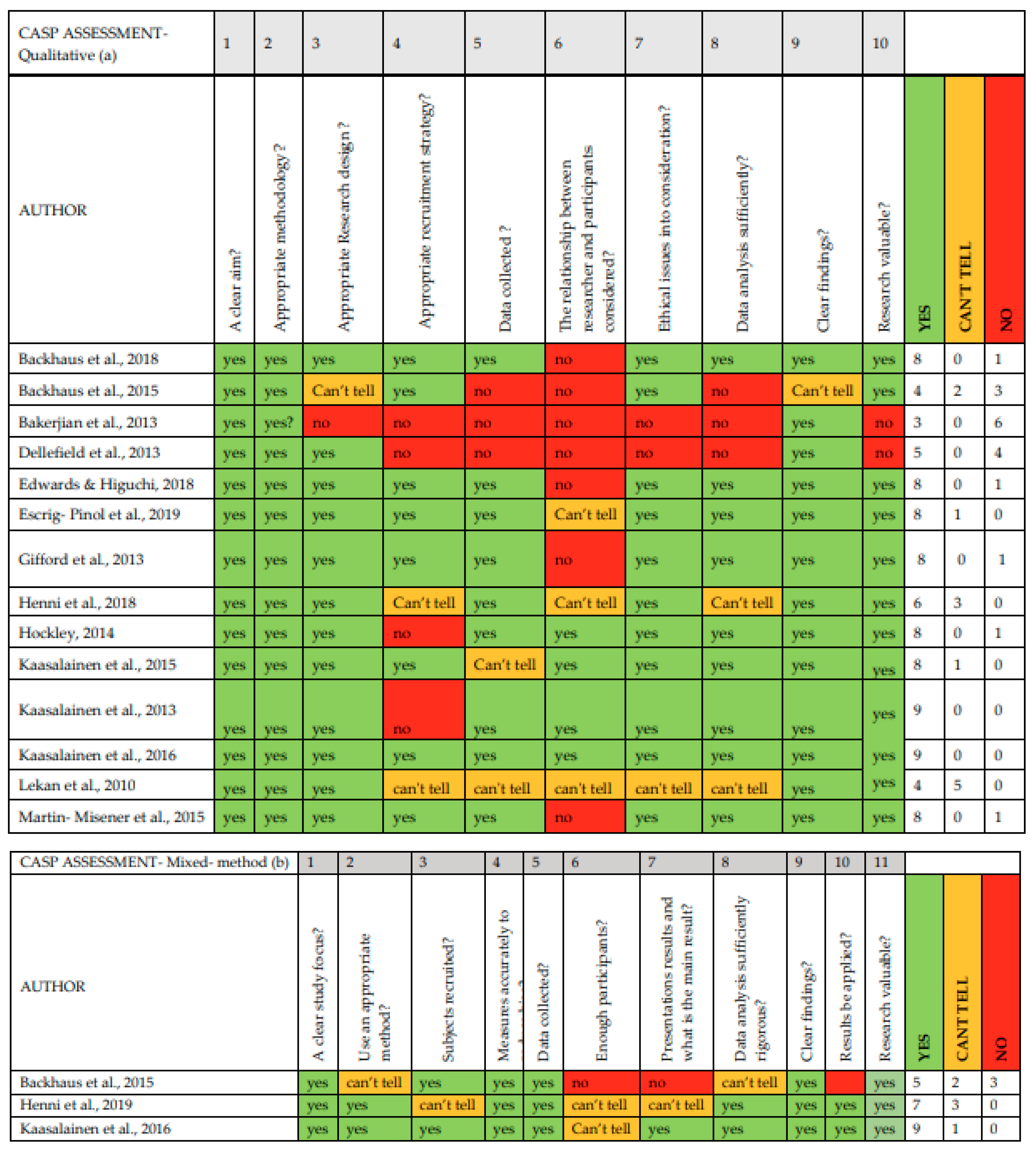
2.4. Quality Appraisal
2.5. Data Analysis
3. Results
3.1. Description of Included Studies
3.2. Competencies
3.2.1. Facilitating Learning Cultures in Nursing Practice
Facilitating Team Reflection on Care Practice
“It [the reflective debriefing groups, led by a nurse specialist] gave scope for reflection on practice and provided a safe environment for staff to make their views known”.[43]
“Because there was this sense of analyzing and reflecting back on a resident’s death, staff in the groups (including myself [NP]) were gradually beginning to critically analyze a number of assumptions and issues about end-of-life care”.[43]
Educating and Training Staff at Formal Moments
“During class sessions [heart failure education], oral and written quizzes were used periodically to stimulate discussion, generate interest, and reinforce learning”.[44]
“The nurse practitioner developed a case study (for discussion at a pain team meeting) to work through pain protocol and enhance application of knowledge and problem-solving ability”.[45]
Educating and Training Staff on the Job
“On-the-job skill competency evaluation was conducted by the Geriatric Advanced Practice Nurse to verify learning, answer questions, review Heart Failure worksheets and provide affirmation and positive feedback”.[44]
“The effect it has when the BN and direct care staff members look together at the client: ’What do you see? What do I see?’ and that you talk about it. Taking five minutes of your time for that [Board member, organization A, respondent 4]”.[46]
3.2.2. Facilitating Effective Work Relationships within Teams
“According to staff, the collaborative environment and the quality of relationships remained constant regardless of age or seniority, and they [nurse supervisor] facilitated the integration of new nurse and personal support workers [PSW] hires”.[47]
“Nursing and interprofessional team members described how the nurse practitioner ‘includes the whole team’, so that each team member was ‘doing [their] piece and all working towards the same goals”.[48]
“Participants spoke about how the type of relationship they had with the nurse practitioners or clinical nurse specialist facilitated knowledge transfer related to implementing the pain protocol. They said that the clinical nurse specialist and nurse practitioners were dedicated to the topic and positive about the change, which facilitated buy-in and motivated staff”.[45]
3.2.3. Facilitating Leadership Capability within Teams
Providing Autonomy; Encouraging Staff to Apply Their Knowledge, Skills and Capacity
“The director of nursing [DON] can provide the vision to inspire the rest of the team, model the appropriate behavior, and encourage others to take leadership positions”.[49]
“Celebrating successful improvements reinforces doing the right thing and encourages staff to continue and sustain the improvement processes”.[49]
“…she usually tries to find me [licensed nurse] throughout the building……..”. And it gives you a good feeling too because she’s [MN] also building the morale staff wise as well. She’s giving you that confidence to go on and continue”.[50]
Facilitating Conditions for Team Performance
“At the ward level, they [board members of organizations] expected BNs to fulfil an informal, clinical leadership role for direct care staff and helping teams to implement care innovations”.[46]
“The director of nursing [DON] can work with the nursing home administrator [bachelor or master educated] to ensure that the quality improvement team [registered nurses] receives the management support and resources necessary to enable success”.[49]
3.2.4. Facilitating Implementation of Guidelines, Standards, and Protocols
Facilitating the Implementation of Evidence-Based Quality Improvement
“As a registered nurse leader, the director of nursing [DON] can provide functional management and oversight of the quality improvement project by assigning appropriate staff to participate in quality improvement as well as identify priority areas that need improvement”.[49]
“The clinical nurses and nurse practitioner used a variety of strategies to help implement the pain protocol in long-term care. They were seen as change champions and active in organizing and facilitating interdisciplinary practice to reinforce the pain protocol and provide ’check-ins’ with staff to identify barriers to implementation”.[45]
“The clinical nurses and nurse practitioners were responsible for organizing and facilitating monthly interdisciplinary pain team meetings with staff to help implement the pain protocol and problem solve issues together”.[45]
Facilitating Various Strategies to Maintain Improvement
“For the quality improvement team, the director of staff development [DSD] can help to identify evidence-based practices and provide staff education about the particular quality improvement intervention, depending on their [quality improvement team] licensure and skill set”[49]
“The nurse practitioner developed a case study (for discussion at a pain team meeting) to work through pain protocol and enhance application of knowledge and problem-solving ability”.[45]
3.2.5. Facilitating a Work Environment to Acknowledge Grief and Loss of Residents within Teams
“NPs also provide support to other LTC staff in terms of their own bereavement when a resident dies. An administrator stated that the NP ‘spends time with the staff in debriefing, and works with the staff’ to help them come to terms with the loss, particularly when the death was difficult”.[50]
“…the Reflective debriefing groups [led by a nurse specialist] fulfilled both a supportive and communicative role among team members. Many staff benefited from being able to open up about personal losses”.[43]
4. Discussion
- Study Limitations
- Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bähler, C.; Huber, C.A.; Brüngger, B.; Reich, O. Multimorbidity, health care utilization and costs in an elderly community-dwelling population: A claims data based observational study. BMC Health Serv. Res. 2015, 15, 23. [Google Scholar] [CrossRef] [PubMed]
- Grover, S. Multimorbidity in the elderly: Are we prepared for it! J. Geriatr. Ment. Health 2019, 6, 35. [Google Scholar] [CrossRef]
- Ng, R.; Lane, N.; Tanuseputro, P.; Mojaverian, N.; Talarico, R.; Wodchis, W.P.; Bronskill, S.E.; Hsu, A.T. Increasing Complexity of New Nursing Home Residents in Ontario, Canada: A Serial Cross-Sectional Study. J. Am. Geriatr. Soc. 2020, 68, 1293–1300. [Google Scholar] [CrossRef] [PubMed]
- United Nations Department of Economic and Social Affairs. Revision of the World Urbaniation Prospects; United Nations Department of Economic and Social Affairs: New York, NY, USA, 2014; Available online: https://www.un.org/en/development/desa/publications/2014-revision-world-urbanization-prospects.html (accessed on 1 November 2021).
- Peters, V.J.T.; Meijboom, B.R.; Bunt, J.E.H.; Bok, L.A.; Van Steenbergen, M.W.; De Winter, J.P.; De Vries, E. Providing person-centered care for patients with complex healthcare needs: A qualitative study. PLoS ONE 2020, 15, e0242418. [Google Scholar] [CrossRef]
- Koren, M.J. Person-Centered Care For Nursing Home Residents: The Culture-Change Movement. Health Aff. 2010, 29, 312–317. [Google Scholar] [CrossRef]
- McCance, T.; McCormack, B.; Slater, P.; McConnell, D. Examining the Theoretical Relationship between Constructs in the Person-Centred Practice Framework: A Structural Equation Model. Int. J. Environ. Res. Public Health 2021, 18, 13138. [Google Scholar] [CrossRef]
- Kitson, A.; Carr, D.; Conroy, T.; Feo, R.; Grønkjær, M.; Waal, G.H.-D.; Jackson, D.; Jeffs, L.; Merkley, J.; Athlin, A.M.; et al. Speaking Up for Fundamental Care: The ILC Aalborg Statement. BMJ Open 2019, 9, e033077. [Google Scholar] [CrossRef]
- Eklund, J.H.; Holmström, I.K.; Kumlin, T.; Kaminsky, E.; Skoglund, K.; Höglander, J.; Sundler, A.J.; Condén, E.; Meranius, M.S. “Same same or different?” A review of reviews of person-centered and patient-centered care. Patient Educ. Couns. 2019, 102, 3–11. [Google Scholar] [CrossRef]
- Phelan, A.; McCormack, B.; Dewing, J.; Brown, D.; Cardiff, S.; Cook, N.; Dickson, C.; Kmete, S.; Lorber, M.; Magowan, R.; et al. Review of developments in person-centred healthcare. Int. Pract. Dev. J. 2020, 10. [Google Scholar] [CrossRef]
- Edvardsson, D.; Sjögren, K.; Lood, Q.; Bergland, D.; Kirkevold, M.; Sandman, P.-O. A person-centred and thriving-promoting intervention in nursing homes- study protocol for the U-Age nursing home multi-centre, non-equivalent controlled group before-after trial. BMC Geriatr. 2017, 17, 22. [Google Scholar] [CrossRef] [Green Version]
- McGilton, K.S.; Bowers, B.J.; Heath, H.; Shannon, K.; Dellefield, M.E.; Prentice, D.; Siegel, E.O.; Meyer, J.; Chu, C.H.; Ploeg, J.; et al. Recommendations From the International Consortium on Professional Nursing Practice in Long-Term Care Homes. J. Am. Med Dir. Assoc. 2016, 17, 99–103. [Google Scholar] [CrossRef]
- Vassbø, T.K.; Kirkevold, M.; Edvardsson, D.; Sjögren, K.; Lood, Q.; Bergland, D. The meaning of working in a person-centred way in nursing homes: A phenomenological-hermeneutical study. BMC Nurs. 2019, 18, 45. [Google Scholar] [CrossRef]
- McCance, T.; Gribben, B.; McCormack, B.; Laird, E.A. Promoting person-centred practice within acute care: The impact of culture and context on a facilitated practice development programme. Int. Pract. Dev. J. 2013, 3, 1–17. [Google Scholar]
- Brekelmans, G.; Maassen, S.; Poell, R.F.; Weststrate, J.; Geurdes, E. Factors influencing nurse participation in continuing professional development activities: Survey results from the Netherlands. Nurse Educ. Today 2016, 40, 13–19. [Google Scholar] [CrossRef] [PubMed]
- McCormack, B.; Dewing, J.; Breslin, L.; Coyne-Nevin, A.; Kennedy, K.; Manning, M.; Peelo-Kilroe, L.; Tobin, C.; Slater, P. Developing person-centred practice: Nursing outcomes arising from changes to the care environment in residential settings for older people. Int. J. Older People Nurs. 2010, 5, 93–107. [Google Scholar] [CrossRef]
- Manley, K.; Sanders, K.; Cardiff, S.; Webster, J. Effective workplace culture: The attributes, enabling factors and consequences of a new concept. Int. Pract. Dev. J. 2011, 1, 1–29. [Google Scholar]
- Hardy, S.; Jackson, C.; Webster, J.; Manley, K. Educating advanced level practice within complex health care workplace environments through transformational practice development. Nurse Educ. Today 2013, 33, 1099–1103. [Google Scholar] [CrossRef]
- Wei, H.; Sewell, K.A.; Woody, G.; Rose, M.A. The state of the science of nurse work environments in the United States: A systematic review. Int. J. Nurs. Sci. 2018, 5, 287–300. [Google Scholar] [CrossRef] [PubMed]
- Ulrich, B.; Cassidy, L.; Barden, M.C.; Varn-Davis, N.; Delgado, M.S.A. National Nurse Work Environments-October 2021: A Status Report. Crit. Care Nurse 2022, e1–e18. [Google Scholar] [CrossRef]
- Bourgault, A.M.; Goforth, C. Embrace Teamwork to Create and Maintain a Positive Workplace Culture. Crit. Care Nurse 2021, 41, 8–10. [Google Scholar] [CrossRef]
- Choi, J.; Kim, D.E.; Yoon, J.Y. Person-Centered Care Environment Associated With Care Staff Outcomes in Long-Term Care Facilities. J. Nurs. Res. 2021, 29, e133. [Google Scholar] [CrossRef]
- Brownie, S.; Nancarrow, S. Effects of person-centered care on residents and staff in aged-care facilities: A systematic review. Clin. Interv. Aging 2013, 8, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Lake, E.T.; Sanders, J.; Duan, R.; Riman, K.A.; Schoenauer, K.M.; Chen, Y. A Meta-Analysis of the Associations Between the Nurse Work Environment in Hospitals and 4 Sets of Outcomes. Med. Care 2019, 57, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Cardiff, S.; Sanders, K.; Webster, J.; Manley, K. Guiding lights for effective workplace cultures that are also good places to work. Int. Pract. Dev. J. 2020, 10, 1–21. [Google Scholar] [CrossRef]
- Manley, K.; O’Keefe, H.; Jackson, C.; Pearce, J.; Smith, S. A shared purpose framework to deliver person-centred, safe and effective care: Organisational transformation using practice development methodology. Int. Pract. Dev. J. 2014, 4, 1–31. [Google Scholar] [CrossRef]
- Manley, K.; Jackson, C. The Venus model for integrating practitioner-led workforce transformation and complex change across the health care system. J. Eval. Clin. Pract. 2020, 26, 622–634. [Google Scholar] [CrossRef]
- Seers, K.; Cox, K.; Crichton, N.J.; Edwards, R.T.; Eldh, A.C.; Estabrooks, C.A.; Harvey, G.; Hawkes, C.; Kitson, A.; Linck, P.; et al. FIRE (facilitating implementation of research evidence): A study protocol. Implement. Sci. 2012, 7, 25. [Google Scholar] [CrossRef]
- van Lieshout, F. Taking Action for Action: A Study of an Interplay between Contextual and Facilitator Characteristics in Developing an Effective Workplace Culture in a Dutch Hospital Setting, through Action Research, in Faculty of Life and Health Science of the University of Ulster in Cooperation with the Knowledge Centre for Implementation and Evaluation of Evidence Based Practice, Fontys University of Applied Sciences; University of Ulster: Belfast, Ireland, 2013. [Google Scholar]
- Williams, C.V. The Role of a Facilitator in Enabling Registered Nurses to Translate Reflective Appraisal into Work-Based Learning and an Evaluation of the Outcomes of this Learning; Queen Margaret University: Edinburgh, Scotland, 2019. [Google Scholar]
- White, E.; Woodford, E.; Britton, J.; Newberry, L.W.; Pabico, C. Nursing practice environment and care quality in nursing homes. Nurs. Manag. 2020, 51, 9–12. [Google Scholar] [CrossRef]
- Canadian Nurses Association. Framework for the Practice of Registered Nurses in Canada 2015; Canadian Nurses Association: Ottawa, ON, Canada, 2014. [Google Scholar]
- Yoo, J.Y.; Kim, J.H.; Kim, J.S.; Kim, H.L.; Ki, J.S. Clinical nurses’ beliefs, knowledge, organizational readiness and level of implementation of evidence-based practice: The first step to creating an evidence-based practice culture. PLoS ONE 2019, 14, e0226742. [Google Scholar] [CrossRef]
- Saunders, H.; Vehviläinen-Julkunen, K. Nurses’ Evidence-Based Practice Beliefs and the Role of Evidence-Based Practice Mentors at University Hospitals in Finland. Worldviews Evid. Based Nurs. 2017, 14, 35–45. [Google Scholar] [CrossRef]
- Lovink, M.H.; Verbeek, F.; Persoon, A.; Waal, G.H.-D.; Smits, M.; Laurant, M.G.H.; van Vught, A.J. Developing an Evidence-Based Nursing Culture in Nursing Homes: An Action Research Study. Int. J. Environ. Res. Public Health 2022, 19, 1733. [Google Scholar] [CrossRef] [PubMed]
- Kowalski, M.O.; Basile, C.; Bersick, E.; Cole, D.A.; McClure, D.E.; Weaver, S.H. What Do Nurses Need to Practice Effectively in the Hospital Environment? An Integrative Review With Implications for Nurse Leaders. Worldviews Evid. Based Nurs. 2020, 17, 60–70. [Google Scholar] [CrossRef] [Green Version]
- Cardiff, S.; McCormack, B.; McCance, T. Person-centred leadership: A relational approach to leadership derived through action research. J. Clin. Nurs. 2018, 27, 3056–3069. [Google Scholar] [CrossRef] [PubMed]
- Tashiro, J.; Shimpuku, Y.; Naruse, K.; Maftuhah; Matsutani, M. Concept analysis of reflection in nursing professional development. Jpn. J. Nurs. Sci. 2013, 10, 170–179. [Google Scholar] [CrossRef]
- Salmond, S.W.; Echevarria, M. Healthcare Transformation and Changing Roles for Nursing. Orthop. Nurs. 2017, 36, 12–25. [Google Scholar] [CrossRef]
- Whittemore, R.; Knafl, K. The integrative review: Updated methodology. J. Adv. Nurs. 2005, 52, 546–553. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Critical Appraisal Skills Program. CASP Checklists. 2022. Available online: https://casp-uk.net/casp-tools-checklists/ (accessed on 1 May 2022).
- Hockley, J. Learning, support and communication for staff in care homes: Outcomes of reflective debriefing groups in two care homes to enhance end-of-life care. Int. J. Older People Nurs. 2014, 9, 118–130. [Google Scholar] [CrossRef] [PubMed]
- Lekan, D.; Hendrix, C.C.; McConnell, E.S.; White, H. The Connected Learning Model for disseminating evidence-based care practices in clinical settings. Nurse Educ. Pract. 2010, 10, 243–248. [Google Scholar] [CrossRef]
- Kaasalainen, S.; Ploeg, J.; Donald, F.; Coker, E.; Brazil, K.; Martin-Misener, R.; Dicenso, A.; Hadjistavropoulos, T. Positioning Clinical Nurse Specialists and Nurse Practitioners as Change Champions to Implement a Pain Protocol in Long-Term Care. Pain Manag. Nurs. 2015, 16, 78–88. [Google Scholar] [CrossRef]
- Backhaus, R.; Verbeek, H.; Van Rossum, E.; Capezuti, E.; Hamers, J.P. Baccalaureate-educated Registered Nurses in nursing homes: Experiences and opinions of administrators and nursing staff. J. Adv. Nurs. 2018, 74, 75–88. [Google Scholar] [CrossRef]
- Escrig-Pinol, A.; Corazzini, K.N.; Blodgett, M.B.; Chu, C.H.; McGilton, K.S. Supervisory relationships in long-term care facilities: A comparative case study of two facilities using complexity science. J. Nurs. Manag. 2019, 27, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Martin-Misener, R.; Donald, F.; Wickson-Griffiths, A.; Akhtar-Danesh, N.; Ploeg, J.; Brazil, K.; Kaasalainen, S.; McAiney, C.; Carter, N.; Martin, L.S.; et al. A mixed methods study of the work patterns of full-time nurse practitioners in nursing homes. J. Clin. Nurs. 2015, 24, 1327–1337. [Google Scholar] [CrossRef]
- Bakerjian, D.; Zisberg, A. Applying the Advancing Excellence in America’s Nursing Homes Circle of Success to improving and sustaining quality. Geriatr. Nurs. 2013, 34, 402–411. [Google Scholar] [CrossRef]
- Kaasalainen, S.; Ploeg, J.; McAiney, C.; Martin, L.S.; Donald, F.; Martin-Misener, R.; Brazil, K.; Taniguchi, A.; Wickson-Griffiths, A.; Carter, N.; et al. Role of the nurse practitioner in providing palliative care in long-term care homes. Int. J. Palliat. Nurs. 2013, 19, 477–485. [Google Scholar] [CrossRef]
- Backhaus, R.; Verbeek, H.; van Rossum, E.; Capezuti, E.; Hamers, J.P. Future distinguishing competencies of baccalaureate-educated registered nurses in nursing homes. Geriatric Nurs. 2015, 36, 438–444. [Google Scholar]
- Dellefield, M.E.; Kelly, A.; Schnelle, J.F. Quality assurance and performance improvement in nursing homes: Using evidence-based protocols to observe nursing care processes in real time. J. Nurs. Care Qual. 2013, 28, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Edwards, N.C.; Higuchi, K.S. Process evaluation of a participatory, multimodal intervention to improve evidence-based care in long-term care settings. Worldviews Evid. Based Nurs. 2018, 15, 361–367. [Google Scholar] [CrossRef]
- Henni, S.H.; Kirkevold, M.; Antypas, K.; Foss, C. The role of advanced geriatric nurses in Norway: A descriptive exploratory study. Int. J. Older People Nurs. 2018, 13, e12188. [Google Scholar] [CrossRef]
- Henni, S.H.; Kirkevold, M.; Antypas, K.; Foss, C. The integration of new nurse practitioners into care of older adults: A survey study. J. Clin. Nurs. 2019, 28, 2911–2923. [Google Scholar] [CrossRef]
- Kaasalainen, S.; Wickson-Griffiths, A.; Akhtar-Danesh, N.; Brazil, K.; Donald, F.; Martin-Misener, R.; DiCenso, A.; Hadjistavropoulos, T.; Dolovich, L. The effectiveness of a nurse practitioner-led pain management team in long-term care: A mixed methods study. Int. J. Nurs. Stud. 2016, 62, 156–167. [Google Scholar] [CrossRef] [PubMed]
- Gifford, W.A.; Davies, B.L.; Ploeg, J.; Eldred, S.; Bajnok, I. Moving Knowledge to Action: A Qualitative Study of the Registered Nurses’ Association of Ontario Advanced Clinical Practice Fellowship Program. Nurs. Leadersh. 2013, 26, 32–57. [Google Scholar] [CrossRef] [PubMed]
- Bengtsson, M. How to plan and perform a qualitative study using content analysis. Nurs. Open 2016, 2, 8–14. [Google Scholar] [CrossRef] [Green Version]
- Heinen, M.; Van Oostveen, C.; Peters, J.; Vermeulen, H.; Huis, A. An integrative review of leadership competencies and attributes in advanced nursing practice. J. Adv. Nurs. 2019, 75, 2378–2392. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.S.; McCormack, B.; Fitzsimons, D.; Spirig, R. Evaluation of a clinical leadership programme for nurse leaders. J. Nurs. Manag. 2012, 20, 72–80. [Google Scholar] [CrossRef]
- Giddens, J. Transformational leadership: What every nursing dean should know. J. Prof. Nurs. 2018, 34, 117–121. [Google Scholar] [CrossRef]
- Silva, J.A.M.; Agreli, H.F.; Harrison, R.; Peduzzi, M.; Mininel, V.A.; Xyrichis, A. Collective leadership to improve professional practice, healthcare outcomes, and staff well-being. Cochrane Database Syst. Rev. 2021, 1, CD013850. [Google Scholar]
- West, M.A.; Lyubovnikova, J.; Eckert, R.; Denis, J.L. Collective leadership for cultures of high quality health care. J. Organ. Eff. People Perform. 2014, 1, 240–260. [Google Scholar] [CrossRef]
- Bishop, C.E. High-Performance Workplace Practices in Nursing Homes: An Economic Perspective. Gerontologist 2014, 54, S46–S52. [Google Scholar] [CrossRef]
- Warrick, D. Developing organization change champions. OD Pract. 2009, 41, 14–19. [Google Scholar]
- Gerrish, K.; Guillaume, L.; Kirshbaum, M.; McDonnell, A.; Tod, A.; Nolan, M. Factors influencing the contribution of advanced practice nurses to promoting evidence-based practice among front-line nurses: Findings from a cross-sectional survey. J. Adv. Nurs. 2011, 67, 1079–1090. [Google Scholar] [CrossRef]
- Goldstein, K.M.; Vogt, D.; Hamilton, A.; Frayne, S.M.; Gierisch, J.; Blakeney, J.; Sadler, A.; Bean-Mayberry, B.M.; Carney, D.; DiLeone, B.; et al. Practice-based research networks add value to evidence-based quality improvement. Healthcare 2018, 6, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Cranley, L.; Cummings, G.G.; Profetto-McGrath, J.; Toth, F.; Estabrooks, C. Facilitation roles and characteristics associated with research use by healthcare professionals: A scoping review. BMJ Open 2017, 7, e014384. [Google Scholar] [CrossRef]
- Vermeulen, H. Evidence-based quality improvement. Ned. Tijdschr Evid. Based Pract. 2014, 123. [Google Scholar] [CrossRef]
- Marcella, J.; Kelley, M.L. “Death is part of the job” in long-term care homes: Supporting direct care staff with their grief and bereavement. Sage Open 2015, 5, 2158244015573912. [Google Scholar] [CrossRef] [Green Version]
- Choi, J.; Flynn, L.; Aiken, L.H. Nursing Practice Environment and Registered Nurses’ Job Satisfaction in Nursing Homes. Gerontologist 2012, 52, 484–492. [Google Scholar] [CrossRef] [PubMed]
- Keene, E.; Hutton, N.; Hall, B.; Rushton, C. Bereavement debriefing sessions: An intervention to support health care professionals in managing their grief after the death of a patient. Pediatr. Nurs. 2010, 36, 185–189. [Google Scholar]
- Raemer, D.; Anderson, M.; Cheng, A.; Fanning, R.; Nadkarni, V.; Savoldelli, G. Research Regarding Debriefing as Part of the Learning Process. Simul. Healthc. 2011, 6, S52–S57. [Google Scholar] [CrossRef]
- Sawyer, T.; Eppich, W.; Brett-Fleegler, M.; Grant, V.; Cheng, A. More Than One Way to Debrief: A Critical Review of Healthcare Simulation Debriefing Methods. Simul. Healthc. 2016, 11, 209–217. [Google Scholar] [CrossRef]
- Yu, F.; Raphael, D.; Mackay, L.; Smith, M.; King, A. Personal and work-related factors associated with nurse resilience: A systematic review. Int. J. Nurs. Stud. 2019, 93, 129–140. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Inclusion | Exclusion |
|---|---|
|
|
| No. | Author(s), Year, Country | Title | Aim Study | Object of Study | Methodology | Participants |
|---|---|---|---|---|---|---|
| 1 | Backhaus et al., 2018 [46]; the Netherlands | Baccalaureate-educated Registered Nurses in nursing homes: Experiences and opinions of administrators and nursing staff | To understand how nursing homes employed BRNs and how they viewed the unique contributions of BRNs for staff and residents in their organizations. | Bachelor registered nurse, EQF 6. |
| Board members, directors, ward/nursing home managers, and BRNs: N = 26 individual interviews and 3 group interviews (N = 14). |
| 2 | Backhaus et al., 2015 [51]; the Netherlands | Future distinguishing competencies of baccalaureate-educated registered nurses in nursing homes | To obtain insight into the competencies, which should in the future distinguish BRNs from other nursing staff in nursing homes. | Bachelor registered nurse, EQF 6. |
| N = 41 experts (no BNs were included) from various countries. |
| 3 | Bakerjian & Zisberg, 2013 [49]; the U.S. | Applying the Advancing Excellence in America’s Nursing Homes Circle of Success to improving and sustaining quality | To describe the potential roles and responsibilities of registered nurse leaders in NHs in implementing and sustaining a comprehensive improvement program. | Nursing leaders: RN’s and director of nursing (DON) and director of staff development (DSD), EQF 4–6. |
| 1 DON; 1 DSD; 1 team leader; 1 APN from a local university; 1 quality improvement (QI) consultant. |
| 4 | Dellefield et al., 2013 [52]; the U.S. | Quality assurance and performance improvement in nursing homes: Using evidence-based protocols to observe nursing care processes in real time. | To describe quality assurance and performance improvement (QAPI) elements and explain how to collect data using direct observation and evidence-based measures and protocols in a QAPI program. | Registered nurses, EQF unknown. |
| Registered nurses and other nursing staff (Nursing assistants). |
| 5 | Edwards & Smith Higuchi, 2018 [53]; Canada | Process evaluation of a participatory, multimodal intervention to improve evidence-based care in long-term care settings | To examine the effect of a multimodal, participatory intervention aimed at improving evidence-based care for the residents of LTC homes. | Best practice Coordinator (BPC); master or bachelor degree. Nurse external facilitator. EQF: 6–7. |
| Staff members: registered and non-registered staff and other health members. Different disciplines, levels, and departments of the LTC sites. External facilitator, nurse facilitator, and best practice coordinator. N = 44 at midpoint and N = 69 at endpoint. |
| 6 | Escrig-Pinol et al., 2019 [47]; Canada | Supervisory relationships in long-term care facilities: A comparative case study of two facilities using complexity science | To seek a better understanding of the factors that contribute to effective supervisory performance in LTCFs. | Nurse supervisor (RN or RPN) as participants, EQF: 6 |
| Two LTCFs: Case-study 1: N = 10 Case-study 2: N = 10 including management (n = 6) (administrators, directors of care and middle managers staff), RNs, and RPNs (n = 7) and PSWs (n = 7). |
| 7 | Henni et al., 2018 [54]; Norway | The role of advanced geriatric nurses in Norway: A descriptive exploratory study | To describe the experience of nurses with their new role as AGNs in care of older adults, and to determine what strategies the AGNs consider important in the development of their new role. | Advanced Geriatric Nurses, EQF: 7 |
| 21 AGNs graduated from the University of Oslo before summer 2016. |
| 8 | Henni et al., 2019 [55]; Norway | The integration of new nurse practitioners into care of older adults: A survey study | To investigate the level of integration of AGNs in their fields of practice; use of their knowledge and skills to reach their full potential. | Advanced Geriatric Nurses, EQF: 7 |
| AGNs (n = 26) and colleagues (n = 465). |
| 9 | Hockley, 2014 [43]; the U.K. | Learning, support and communication for staff in care homes: outcomes of reflective debriefing groups in two care homes to enhance end-of-life care | 1. To identify problems that staff experience in caring for a resident who is dying and the impact on the provision of high-quality end-of-life. 2. To examine what actions could successfully be implemented in order to promote high-quality end-of-life care. | Nurse specialist in palliative care, as the leading facilitator, EQF: 7 |
| 10 RdBGs, per RdBGs; 34 different staff members attended RdBGs; nurse managers, nurses, and health care assistants (HCA). |
| 10 | Kaasalainen et al., 2015 [45]; Canada | Positioning clinical nurse specialists and nurse practitioners as change champions to implement a pain protocol in long-term care | To explore the role of a clinical nurse specialist and a nurse practitioner as change champions during the implementation of an evidence-based pain protocol in LTC. | Advanced practice nurses: Nurse practitioners (NP) and Clinical nurse specialist (CNS), EQF: 7 |
| 1. APN diaries (first 3 months) completed by CNS and NP. 2. Participant observation (36 h): research assistant shadowed each CNS and NP. 3. Four focus group at the end of implementation phase: 2 with PSWs (n = 17) and 2 with RPNs and RNs (N = 11), Individual interviews: members of administration (N = 5) and interdisciplinary team members (N = 4) and the NP and CNS. |
| 11 | Kaasalainen et al., 2013 [50]; Canada | Role of the nurse practitioner in providing palliative care in long-term care homes | To present study findings about the role of the NP in providing palliative care in long-term care homes (LTCs). | Nurse practitioners, EQF: 7 |
| Physicians (n = 9), licensed nurses (n = 20), PSW or healthcare aides (n = 15), managers (n = 19), RN managers or leaders (n = 10), allied health care providers (n = 31), NPs (n = 4), residents (n = 14), and family members (n = 21). N = 143 were interviewed individually or in a focus group; 35 focus groups and 25 individual interviews. |
| 12 | Kaasalainen et al., 2016 [56]; Canada | The effectiveness of a nurse practitioner-led pain management team in long-term care: A mixed methods study | 1. To evaluate an NP-led, IP pain management team in LTC. 2. To evaluate the effectiveness of the implementation of the NP-led pain management team in improving resident outcomes and health-care provider outcomes. 3. To explore staff perceptions of the implementation of the NP-led pain management team. | Nurse practitioners, EQF: 7 |
| Total: 139 residents full intervention group; 108 residents to partial intervention group and 98 residents in control group. |
| 13 | Lekan et al., 2010 [44]; U.S. | The Connected Learning Model for disseminating evidence-based care practices in clinical settings | To describe the development, implementation and feasibility evaluation of the Connected Learning Model to facilitate adoption of heart failure clinical practice guidelines for symptom recognition in one nursing home. | Advance practice nurse as the facilitator, EQF: 7 |
| Four nursing units staffed with: RN, LPN, NA nursing staff and RN supervisor (n = unknown). Evaluation of the feasibility of different teaching–learning strategies and on-the-job skill competency evaluation to verify learning. |
| 14 | Martin-Misener et al., 2015 [48]; Canada | A mixed methods study of the work patterns of full-time nurse practitioners in nursing | To explore the integration of the NP role in Canadian nursing home settings to enable the full potential of this role to be realised for resident and family care. | Nurse practitioner, EQF: 7 |
| Survey: Nurse practitioners (N = 26). Case-study: healthcare providers, administrators, family members, multidisciplinary health professionals, NPs, managers, physicians, residents, and unregulated care staff were interviewed via individual interview or focus group (N = 150). |
| 15 | McGilton et al., 2016 [12]; International | Recommendations From the International Consortium on Professional Nursing Practice in Long-Term Care Homes | 1. To describe recommendations about priority issues for action and a research agenda regarding the RN in LTCHs. 2. To reach consensus on priority issues future research. | Registered nurses, EQF: unknown. |
| Consortium: Nursing experts engaged in research, policy, administration/operations, and education in aging and LTC. |
| 16 | Gifford et al., 2013 [57]; Canada | Moving Knowledge to Action: A Qualitative Study of the Registered Nurses’ Association of Ontario Advanced Clinical Practice Fellowship Program | To describe the perceptions of Advanced Clinical Practice Fellowship (ACPF) fellows regarding their influence on quality of care and patient outcomes through advanced nursing knowledge translation and skills development. | Masters prepared nurses, EQF: 7 |
| Primary mentors of the ACPF fellows. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Handor, R.; Persoon, A.; van Lieshout, F.; Lovink, M.; Vermeulen, H. The Required Competencies of Bachelor- and Master-Educated Nurses in Facilitating the Development of an Effective Workplace Culture in Nursing Homes: An Integrative Review. Int. J. Environ. Res. Public Health 2022, 19, 12324. https://doi.org/10.3390/ijerph191912324
Handor R, Persoon A, van Lieshout F, Lovink M, Vermeulen H. The Required Competencies of Bachelor- and Master-Educated Nurses in Facilitating the Development of an Effective Workplace Culture in Nursing Homes: An Integrative Review. International Journal of Environmental Research and Public Health. 2022; 19(19):12324. https://doi.org/10.3390/ijerph191912324
Chicago/Turabian StyleHandor, Rachida, Anke Persoon, Famke van Lieshout, Marleen Lovink, and Hester Vermeulen. 2022. "The Required Competencies of Bachelor- and Master-Educated Nurses in Facilitating the Development of an Effective Workplace Culture in Nursing Homes: An Integrative Review" International Journal of Environmental Research and Public Health 19, no. 19: 12324. https://doi.org/10.3390/ijerph191912324