Heroin Assisted Treatment (HAT) involves the provision of medical-grade heroin - also called diamorphine - to registered patients as part of a treatment programme. Patients attend a clinic once or twice a day, and use their prescriptions on site, under medical supervision. It is normally for people who have not had success with other treatments.
HAT reduces health problems. No one overdoses or dies, because people are given a carefully measured dose to use. Safer injecting advice, and onsite healthcare, reduce and treat injecting wounds and other health issues. The use of sterile injecting equipment means no infections from needle sharing, including HIV and hepatitis C, occur.
HAT increases take-up and retention in treatment, and substantially reduces or eliminates consumption of illegal heroin, and acquisitive crime and sex work to fund use (reducing money going to organised crime), as well as high-risk street injecting and discarded needles.
Most importantly, extremely vulnerable and marginalised people are having their lives stabilised, and they are not having to steal, beg or use sex work to pay for drugs. This allows them to engage with wrap-around mental health, housing and other support that is also on offer, with huge benefits to them, their families and the communities they live in.
The UK Government supports HAT (for example in its Modern Crime Prevention Strategy) as do its official advisers - the Advisory Council on the Misuse of Drugs (ACMD).
'Central government funding should be provided to support HAT for patients for whom other forms of Opioid Substitution Treatment have not been effective.' Advisory Council on the Misuse of Drugs, 2016
Inside a UK HAT clinic
In this short video, Acting Police and Crime Commissioner Lisa Oldroyd explains why they helped fund the Middlesbrough HAT clinic, and Danny Ahmed walks viewers through how it works.
This briefing gives a very short overview of HAT. For a focus on the crime reduction and policing benefits of HAT, including how it can reduce illegal heroin and crack markets, read this briefing.
The history of HAT
Heroin Assisted Treatment is well established internationally, already legal, and has a long history including in the UK.
The ‘British System’ developed following the 1926 Rolleston Report allowed doctors to prescribe heroin to people diagnosed as dependent on it, for take home use, so they would not be buying heroin of unknown strength from the criminal market. Doctors were later required to obtain a specific Home Office Licence. Particularly following the introduction of the Misuse of Drugs Act (MDA) in 1971, this system of take-home prescribing was much reduced, with an increasing focus on treatment clinics primarily aimed at making people abstinent. Although some continued to prescribe heroin, for example the drug dependency clinic of London’s University College Hospital.
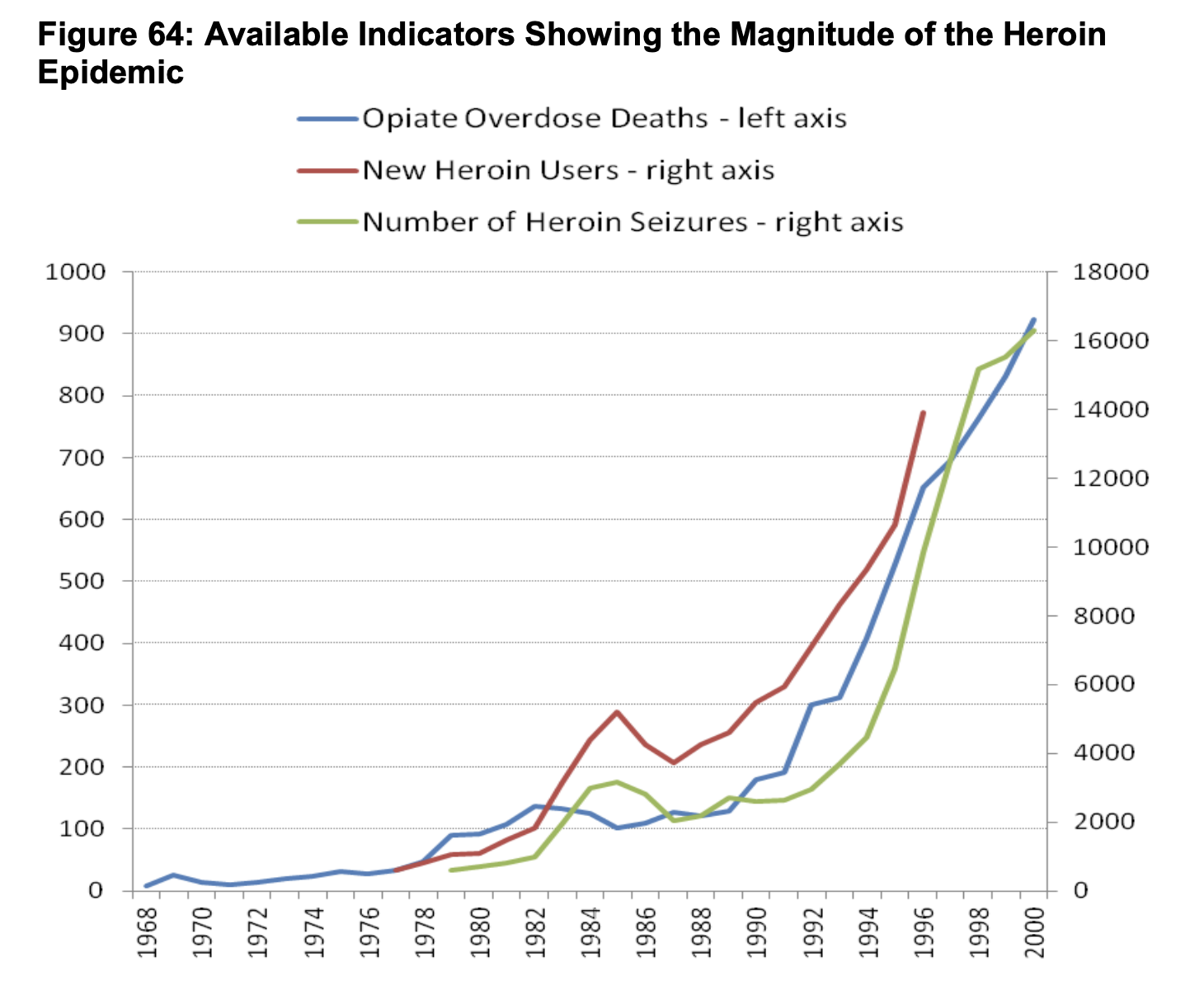
Taking a more punitive approach, underpinned by the MDA, was not successful, with numbers dependent on heroin spiralling, along with overdose deaths, and other harms to individuals and society.
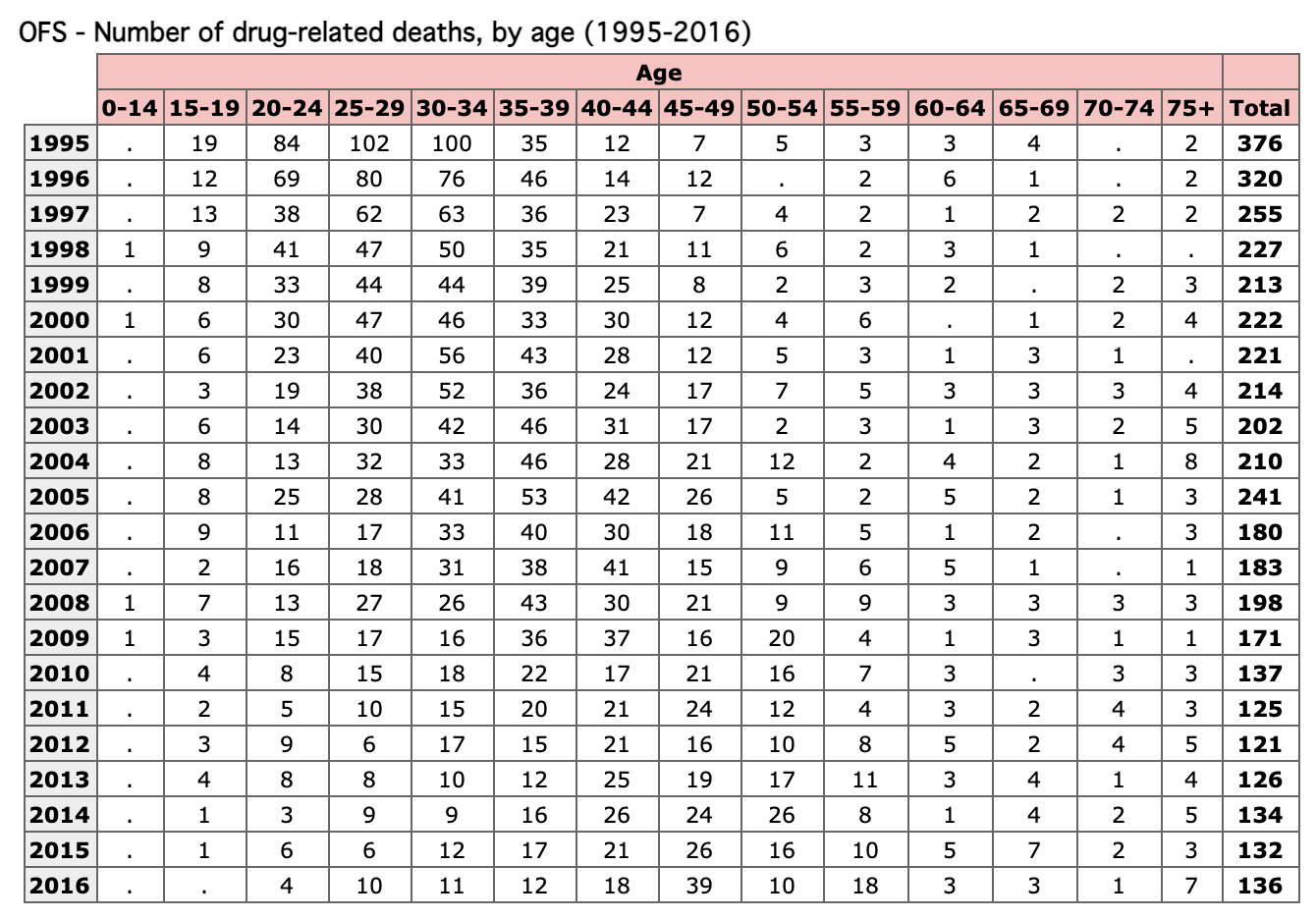
This is worth comparing with what happened to drug related deaths (mainly opiate) in Switzerland after they moved to a health-led approach, including HAT and Safer Drug Consumption Rooms.
In 1982, Dr John Marks started prescribing heroin (along with injectable and oral methadone) in the North West of England as a maintenance approach. It aimed to keep people alive, and reduce health and social harms they were suffering, with the intention of allowing them to move on from heroin use in their own time. It was also expressly about reducing money going to organised crime groups, and as such was a challenge to the prohibitionist idea that the only way to restrict illegal drug markets was through enforcement. Marks initially prescribed injectable heroin, and later heroin injected into cigarettes to smoke. Despite clear benefits, Dr Marks was eased out of his job, and his clinics shut in the early 1990s as a result of the ongoing moral panic about heroin, and opposition from some politicians locally and from the Home Office as his work became nationally and internationally famous.
Not, however, before Swiss experts visited Marks to learn about his approach, and ‘The British System’.
Ex-Swiss President Ruth Dreifuss explains to UK Police Commissioners how Dr Marks work contributed to Swiss HAT Clinics
As a result, the first Swiss pilot HAT clinics opened in 1994. In 1997, the federal government approved a large-scale expansion, aimed at 15% of the nation’s estimated 30,000 people who use heroin who had not succeeded with other treatments. The programme soon won strong support from the public, being backed in multiple local and national referendums.
Police and Crime Commissioners Ron Hogg and Arfon Jones in a Geneva HAT Clinic
So when the UK opened three successful ‘pilot’ NHS supervised injecting clinics (London, Brighton and Darlington) in 2009 - the Randomised Injectable Opiate Treatment Trial (RIOTT) - they were retreading ground long established in the UK and elsewhere. The last of the RIOTT clinics shut when the Department of Health withdrew funding in 2016 because of austerity related cuts. In 2019 HAT clinics in Glasgow and Middlesbrough opened, with widespread interest elsewhere in the UK. In January 2021 the Scottish Government announced its intention to roll HAT out nationwide.
For more details on the rationale for, and the process involved, in opening the Middlesbrough HAT clinic, and its very promising early outcomes, see this presentation by its manager Daniel Ahmed.
Take-home HAT
Historically, heroin was prescribed for take-home use in the UK, although such provision has been dramatically scaled back since the 1970s. Around 250 people in 24 areas still receive this treatment, with no evidence of diversion into the illegal market. For established clients of HAT clinics, where supervision is no longer needed, or where supervised use is not an option, an expansion of this service could be made available where clinically appropriate.
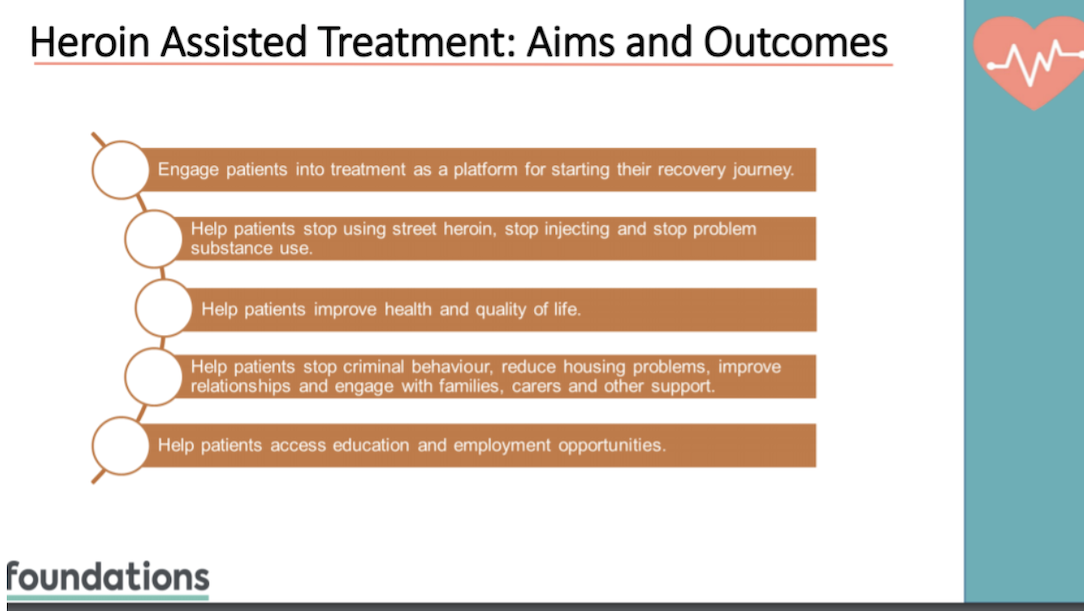
Aims and Outcomes
Daniel Ahmed, the Middlesbrough HAT Clinic Manager summarises the aims of HAT as follows:
Improving Health
HAT delivers the health benefits of prescribed supply - heroin of known strength, free from contaminants and adulterants, used with clean injecting equipment - but combined with the benefits of supervised use in a safe and hygienic venue. So HAT clinics prevent overdose and HIV infection, provide regular access or referral to counselling, social, health-care and treatment services, while preventing diversion of prescribed heroin to the illicit market.
Studies looking at long term impacts, found that after 6 years, over half of clients were no longer being prescribed heroin. Both those still in the programme, and those who had left it, had maintained their reductions in illegal drugs use, and illegal income, with sustained improvements in most social variables.
These positive outcomes have been widely reproduced, including in all UK trials and current clinics. Reviews by the Cochrane Collaboration and the European Monitoring Centre for Drugs and Drug Addiction(EMCDDA) concluded that HAT can lead to substantially improved health and wellbeing, and marked improvements in social functioning e.g. stable housing and a higher employment rate.
Reducing Illegal Heroin Use and Organised Crime Income
In Switzerland, research suggests that the 10-15% of people eligible for HAT were using 30-60% of all illegal heroin. This is in line with other drug use patterns e.g. the 4% heaviest drinkers in the UK provide 23% of alcohol industry revenue, and the 25% heaviest some 68% of revenue. Taking this very high-using segment of their customer base away from organised criminals could significantly reduce their income, and related harms, from the drugs market.
The UK trials of HAT found three quarters of those prescribed heroin substantially reduced use of ‘street’ heroin. Of these, three quarters remained almost, or completely abstinent. This is remarkable in a group for whom daily illicit use - even while in treatment - was the norm. Clients were spending an average of just over £300 a week on illegal drugs before entering the UK trial. This reduced to under £50 a week at 6 months. For the 40 people on the RIOTT trial, total spend fell from £14k a week to £2k per week. So if replicated, 50 people in HAT (the number planned longer term for Glasgow’s pilot) could reduce illegal drug revenue by £780k per year. If the UK introduced HAT at the levels in Switzerland (where ~6% of the heroin using population is in HAT at any given point) that would equate to around 18k patients, taking about £281 million a year from the illegal heroin market.
Swiss research concluded: 'It seems likely that users who were admitted to the program accounted for a substantial proportion of consumption of illicit heroin, and that removing them from the illicit market has damaged the market’s viability.'
Reducing Acquisitive Crime
Reducing use of illegal drugs reduces the pressure to commit crime to pay for them. For example, the 40 people prescribed heroin in the RIOTT trials were committing 1731 self-reported crimes in the 30 days prior to entering treatment. After 6 months, this fell to 547 crimes per month - a two-thirds reduction. A substantial number became ‘crime-abstinent’.
Early evaluation of the Middlesbrough clinic outcomes also suggests pronounced crime reduction effects.
A Rand report on the impact of HAT on crime said of one RIOTT project area: 'Initially, the police thought that a whole cohort of criminals had either died or migrated away from the area because there were people they had seen on a very regular basis – apprehending them for crimes – and suddenly they weren’t on the police radar at all. Because the heroin-assisted treatment was so effective for them in reducing their criminal activity to fund their habit.'
And: 'In Switzerland, one interviewee reported that instances of criminality within the patient group at his HAT clinic had fallen to almost zero. Another reported that the drop in crime has deepened support for the program from police, who generally have a cooperative relationship with clinics'
This supports many similar findings, including that Switzerland saw: 'a substantial fall in criminal involvement... This fall was greatest (50% to 90%) for the most serious offenses, such as burglary, muggings, robbery and drug trafficking.'
While research for the Home Office has noted '[A]ggregate-level change in numbers of heroin/crack users is likely to affect crime trends.' What the above underlines is that it is more correct to say changes in numbers of people using illegal heroin and crack.
Reducing initiation into heroin use
In Swiss trials, 43% of patients entering HAT sold drugs to finance their own use. This fell to 6% after 12 months, a figure confirmed by police data showing an 80% fall in the number of offences participants committed after 24 months. The researchers said that it is likely the programme disrupted the functioning of the market by removing retail workers.
'The workers no longer sold drugs to existing users, and equally important, no longer recruited new users into the market. The heroin prescription market may thus have had a significant impact on heroin markets in Switzerland.” Researchers also concluded: “The harm reduction policy of Switzerland and its emphasis on the medicalisation of the heroin problem seems to have contributed to the image of heroin as unattractive for young people.'
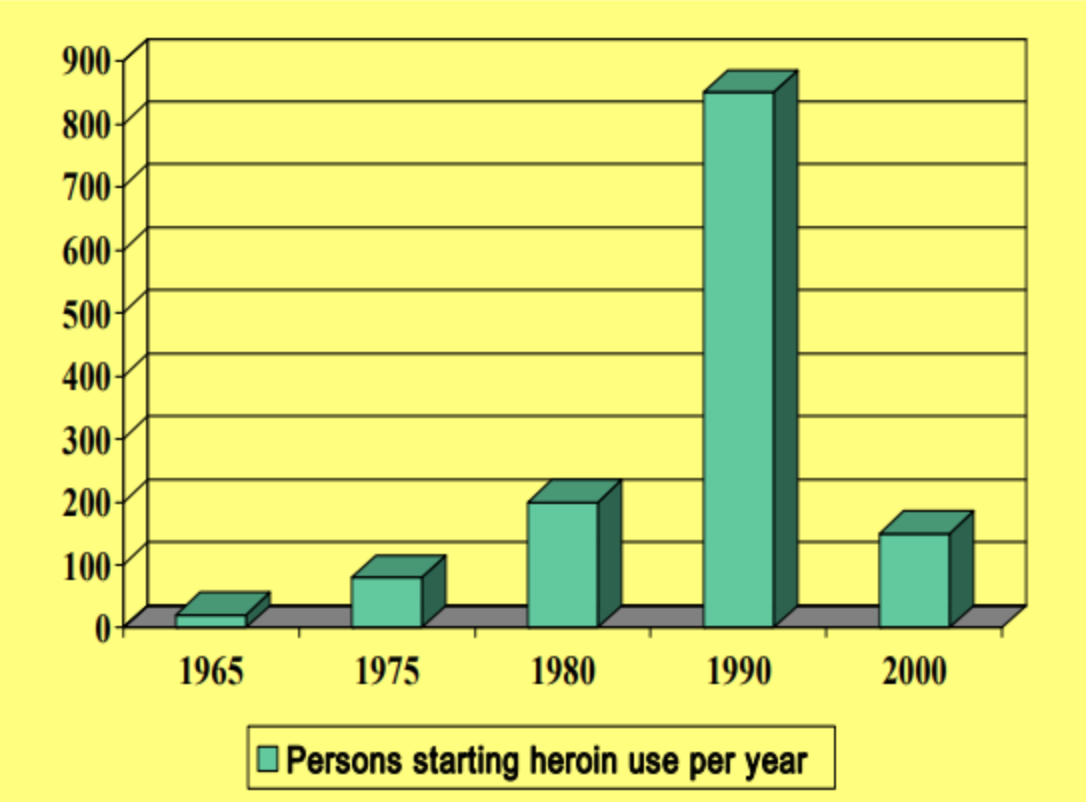
For example, the number of new people using heroin in the Zurich area fell from 850 per year to 150 , and the population of problematic heroin users declined by 4% a year.
Reducing crack use
PHE has said we need to: 'explore more effective methods of getting crack users into treatment and to provide a more attractive treatment offer which is tailored to their specific needs.' A significant proportion of people who use crack are also dependent on heroin. HAT provides an opportunity to address both their heroin and crack use at the same time.
Dr Thilo Beck, who runs Swiss HAT clinics explains how this works: 'HAT is a very effective way to get a population that is otherwise difficult to reach into regular treatment. Once in treatment...marked psycho-bio-social stabilisation occurs. In this context reduction/better control of use of other substances like cocaine is frequently seen.'
For example, as well as almost eliminating illegal heroin use:
Prior to entering the UK RIOTT trials, around three quarters of clients were using crack, while at 6 months this proportion had reduced, as had the amount used
In Switzerland, research found only 15% of new HAT clients had not used crack/cocaine in the previous six months; but the proportion of non-cocaine users increased progressively to 28% six months after admission, 35% after 12 months, and 41% after 18 months
Middlesbrough’s HAT clinic has seen clients reducing crack use by 47%, with other illegal drug use also falling
Numerous studies have demonstrated HAT to be highly cost-effective - as the EMCDDA put it - “HAT saves money”. The high cost per client relative to standard opiate substitution therapy is more than matched by savings across health, criminal justice and other services that cannot be achieved with other treatment options.
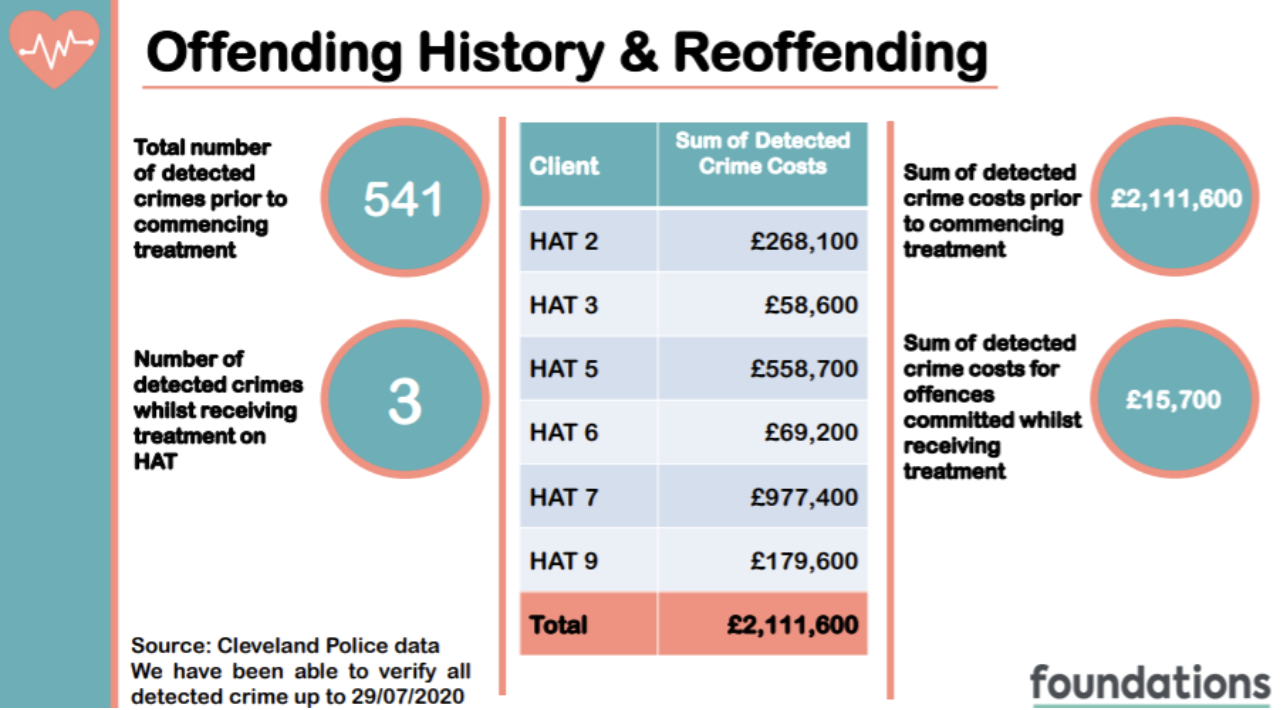
For example, Cleveland Police and Crime Commissioner Barry Coppinger said in support of the cost-effectiveness of introducing HAT to Middlesbrough: 'A prolific cohort of 20 drug-dependent offenders have cost the public purse almost £800,000 over the last two years - and that’s only based on crimes that are detected.' The substantial drop in criminal activity delivered by HAT in Middlesbrough and elsewhere will deliver substantial savings from reduced policing and other criminal justice costs, including court and prisons, as well as savings to the community and businesses.
In 2017, following 75 HIV infections from needle-sharing in 18 months the Glasgow NHS conducted a business case for HAT/ supervised injection facilities: 'Our proposals...would help to address a wide range of issues and so relieve considerable pressure on services elsewhere in the system. The evidence clearly shows the potential for these proposals to create long-term savings and so the economics of this issue are also compelling.' Glasgow NHS put savings to the public purse at more than £940,000 annually in reduced health and social costs.
Given average lifetime treatment cost of £360k per HIV infection, and costs of hepatitis C treatment, even a small reduction in blood-borne infections could make a HAT clinic cost-effective, even before considering reductions in ambulance callouts, overdose and other health related costs, or reductions in crime costs or impacts of street injecting on business and community amenity.
How much does HAT cost?
The budget needed to open a pilot will vary depending on a number of factors. Historically, the cost of clinical-grade heroin was £12-15k per person, but that has been reduced to about £5000 - around 2-3 times the cost of buprenorphine.
Cleveland’s HAT is estimated to be costing around £12k per person annually, with the bulk of the remaining cost beyond the medication being staffing. Running and set up costs can be reduced if an existing facility is used, so sharing costs for premises, admin and other overheads. The cost of wrap around services like housing, social services and mental health provision are not HAT costs - HAT is just providing a gateway to services that should be being provided anyway to this group.
According to the EMCDDA, these costs are similar to those in mainland European countries
The Glasgow HAT clinic is funded by the NHS, while Middlesbrough’s is funded by a coalition of the Police and Crime Commissioner, probation services, prisons, specialist GP, treatment and health services.
Are there downsides?
Concerns that HAT may encourage drug use have proven unfounded. As noted above, it may reduce drug use and initiation. The EMCDDA and other reviews found that rather than patients increasing their heroin doses when given the option, they stabilised and often started reducing them, usually within two or three months, and uptake of other treatments also increased.
It is not viable to have a HAT clinic near everyone who would benefit. Visiting a clinic up to three times a day is a barrier to many kinds of employment, involvement in childcare, or other demands. Where this becomes an issue, the option for take-home use should be considered where risk of diversion of prescribed heroin to the illegal market is deemed low.