
Virus Watch preliminary findings on 24th March 2021
You can find our most recent results at findings so far.
Virus Watch is a research study run by University College London and the NHS. Virus Watch aims to identify how SARS-CoV-2 spreads, and how to stop it. The findings from the Virus Watch study presented on this page are early, preliminary results and should be interpreted with caution. We are presenting these early findings for participants, the general public and policy makers. These early data represent an example of how we will use the results of Virus Watch to identify how SARS-CoV-2 spreads, and how to stop it. A detailed description of the Virus Watch study and our research questions can be found in our study protocol.
Table of contents
- Summary of findings
- Interpretation of findings
- Trends, patterns and psychological influences on COVID-19 vaccination intention
- Household overcrowding and risk of COVID-19
- Prevalence of cough, fever and loss or change to sense of smell and/or taste by week
- Characteristics of people in Virus Watch
1. Summary of findings:
- Virus Watch began recruiting people in June 2020 and as of 24th March 2021, 22,995 households and 47,618 people across England and Wales have joined the study.
- More than four out of five people (86%) of people who were uncertain or intending to refuse a COVID-19 vaccine in December 2020 changed their mind and planned on, or had already accepted, a vaccine in February 2021. This shift was consistent across all ethnic groups and all levels of social deprivation.
- Overcrowded households had twice the risk of PCR confirmed SARS-CoV-2 compared to under-occupied households. People in ‘balanced’ accommodation (where the number of rooms was equal to the number of people) also had an increased risk of PCR confirmed SARS-CoV-2 compared to under-occupied houses.
2. Interpretation of findings
Our findings about vaccination intention suggest that the majority of people, across all ethnic groups and levels of deprivation, who were uncertain about taking, or intended to refuse, a COVID-19 vaccine have now changed their minds. Given this, our findings show the importance of making repeated offers of a COVID-19 vaccine as many people have changed their mind over the course of a few months.
Public health interventions to prevent and stop the spread of SARS-CoV-2 need to consider the unequal burden of risk of being infected for people living in overcrowded households. Addressing England’s overcrowding challenge will likely require a significant increase in the supply of housing and investment in sustainable and high-quality housing will support health, jobs and the wider economic recovery.
3. Trends, patterns and psychological influences on COVID-19 vaccination intention
Public reluctance or refusal to take a vaccine when offered is thought to be a potential threat to the UK’s COVID-19 vaccination programme’s plans to achieve high vaccination coverage across the population. Early evidence of disparities in vaccine intention between ethnic and social groups has led to significant concern among public health practitioners, the NHS (which is leading the UK’s vaccine delivery), voluntary sector organisations, and politicians. Following concerted and targeted action to increase public intention to take a COVID-19 vaccine, it is not yet clear how, or whether, vaccination intention is changing over time in England and Wales.
We asked Virus Watch participants ‘Would you accept a COVID-19 vaccine if offered?’ in December 2020 and again in February 2021. Survey response rate was 56% (20,792/36,998) in December and 52% (20,284/38,727) in February, with 14,713 adults reporting across both time points. Of participants reporting across both timepoints, 13,281 (90%) answered ‘Yes’ and 1,432 (10%) responded ‘No’ or ‘Unsure’ in December 2020. Of those answering ‘No’ or ‘Unsure’ in December 2020, 1,233 (86%) went on to answer ‘Yes’ or ‘Already had a COVID-19 vaccine’ in February 2021. The magnitude of this shift was consistent across all ethnic groups measured. 87% of White British people, 88% of people from Black backgrounds, 90% of people from South Asian backgrounds, 78% of people from White Other backgrounds and 72% of people from Mixed backgrounds who were uncertain or intended to refuse a COVID-19 vaccine in December 2020 went on to change their minds and planned to accept, or had already accepted, a vaccine in February 2021. This shift is also consistent across all levels of social deprivation, ranging from 79% in more deprived areas to 89% in the least deprived areas.
Figure 1. Shift in vaccine intention between December 2020 and February 2021.

Despite these shifts, disparities in vaccine intention still exist. In this study, age was most strongly associated with vaccination intention. For example, we found 25 to 35 year olds were almost 9 times more likely to intend to refuse a Covid-19 vaccine compared to over 75 year olds, after adjusting for other factors such as sex, ethnicity, deprivation and underlying health condition. The association between ethnicity and vaccination intention has weakened, but not disappeared, over time. Both vaccine- and illness-related psychological factors such as concerns about vaccine safety or perceptions around risk of getting ill were shown to influence vaccination intention.
Participation in the Virus Watch study is voluntary and as the sampling is non-random, the cohort is likely biased toward people concerned about COVID-19 and participants may not be representative of the national population. Whilst we found encouraging increases in vaccine confidence, there remains a need to work with communities where uptake rates are low to address concerns and improve accessibility of vaccines.
4. Household overcrowding and risk of SARS-CoV-2
Household overcrowding is associated with increased risk of infectious diseases across cultures and countries. Limited data exist in England and Wales linking household overcrowding and risk of COVID-19. We used data collected from the Virus Watch cohort to examine the association between overcrowded households and COVID-19. We calculated the number of persons per room and classified accommodation as overcrowded when the number of rooms was less than the number of people.
On 16th February 2021, 46,360 participants in the Virus Watch study were invited to take part in the monthly survey. 26,059 Virus Watch participants completed data about their accommodation type enabling calculation of overcrowding status. The proportion of participants with a positive SARS-CoV-2 PCR result was highest in the overcrowded group (5.3%; 56/1,066) and lowest in the under-occupied group (2.3%; 527/22,944). Overcrowded households had twice the risk of PCR confirmed SARS-CoV-2 compared to under-occupied households after we accounted for differences of age, sex, adults living in a household with a child and number of close contacts outside of the household in the last seven days.
Please see this link for our full analysis of household overcrowding and risk of SARS-CoV-2.
5. Prevalence of cough, fever and loss or change to sense of smell and/or taste by week
The prevalence of cough, fever and loss or change to sense of smell and/or taste across all age groups was highest in the week beginning 14th September 2020 at 3,791 per 100,000 (Figure 2). The peak seen in the week commencing 14th September 2020 coincides with a large number people testing positive for Rhinovirus in the Public Health England data mart surveillance results (see Figure 13 in this Public Health England report) in the same time period, suggesting this peak in symptoms of cough, fever and loss or change to sense of smell was likely driven by Rhinovirus and not SARS-CoV-2 (the virus responsible for COVID-19). After declining from this peak, the prevalence of these symptoms began to increase again from week commencing 7th December 2020 and peaked on week commencing 28th December at 1,858 per 100,000 and has declined and then plateaued since with levels at 739 per 100,000 for week commencing 8th March 2021.
Figure 2. Weekly prevalence of cough, fever and loss or change to sense of smell and/or taste per 100,000 people with 95% confidence intervals.

Figure 3. Weekly prevalence of cough, fever and loss or change to sense of smell and/or taste per 100,000 people by age group with 95% confidence intervals.

Notes:
- All results are provisional and subject to revision.
- These statistics refer to symptoms reported by Virus Watch participants in the community.
- Weekly prevalence rates used in these figures were calculated using the total number of people reporting to Virus Watch each week as the denominator, and the number of people reporting symptoms of cough fever and loss of smell or taste as the numerator.
- The date range in Figure 3 is different to Figure 2 in order to focus on the typical ‘cold and flu season’ to see the trends more clearly.
We excluded data from the first week of reporting for all participants.
6. Characteristics of households and individuals in Virus Watch
Virus Watch began recruiting people in June 2020 and as of 24th March 2021, 22,995 households and 47,618 people across England and Wales have joined the study (Table 1). Participants were recruited using a range of methods including sample by post, social media, letters and SMS messages from General Practices.
A total of 814,514 weekly surveys have been completed by Virus Watch participants and completion and retention of participants has been high (Figure 4) with 30,603 completing over 75% of surveys.
Table 1: Participants in Virus Watch, 25th January 2021
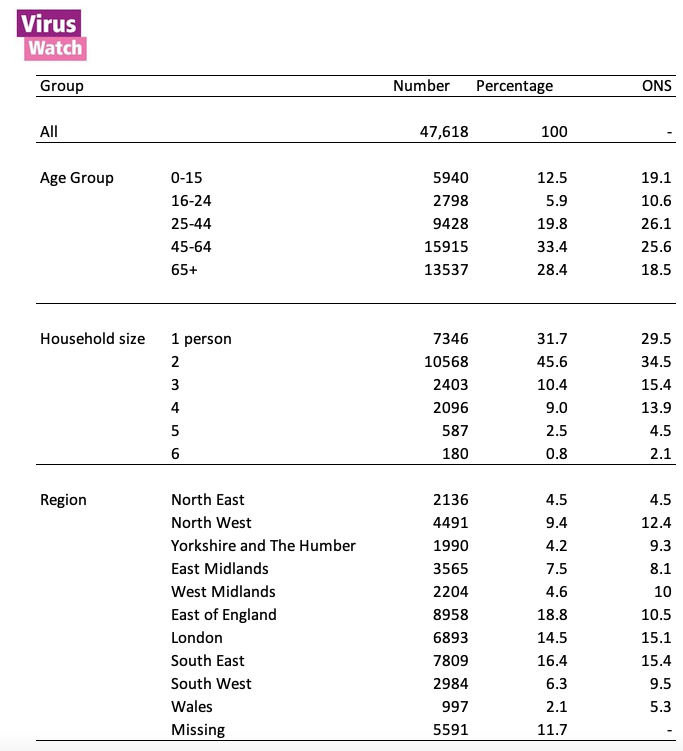
*ONS = Office for National Statistics. ONS data for age and region drawn from Mid-2019 Estimates of the Population for the UK, England, and Wales, Scotland and Northern Ireland (figures for England and Wales). ONS data for household size drawn from Families and Households in the UK 2019 (UK wide estimates).
Figure 4: Count of survey completions by week since start of Virus Watch recruitment in June 2020.

Notes:
- All results are provisional and subject to revision.
- These results exclude participants who did not ever complete a weekly survey (4,419 participants).