
Frailty among Older People during the First Wave of the COVID-19 Pandemic in The Netherlands †

 ,
,
Abstract
:1. Introduction
- Keep a social distance of at least 1.5 m.
- People ≥ 70 years were advised to stay at home and see a maximum of two regular visitors at home.
- Work from home and travel as limited as possible.
- Indoor sports activities were not allowed.
- Shops were open with limited access.
- Hairdressers, restaurants, museums, etc., were closed.
- All activities in community centers were canceled [18].
2. Materials and Methods
2.1. Lifelines COVID-19 Cohort Study
2.2. Participants
2.3. Variables
2.3.1. Groningen Frailty Indicator
2.3.2. Perceived Concerns and Threats Related to the COVID-19 Pandemic
2.3.3. Variables Possibly Associated to Presence of Frailty
2.4. Statistical Analyses
3. Results
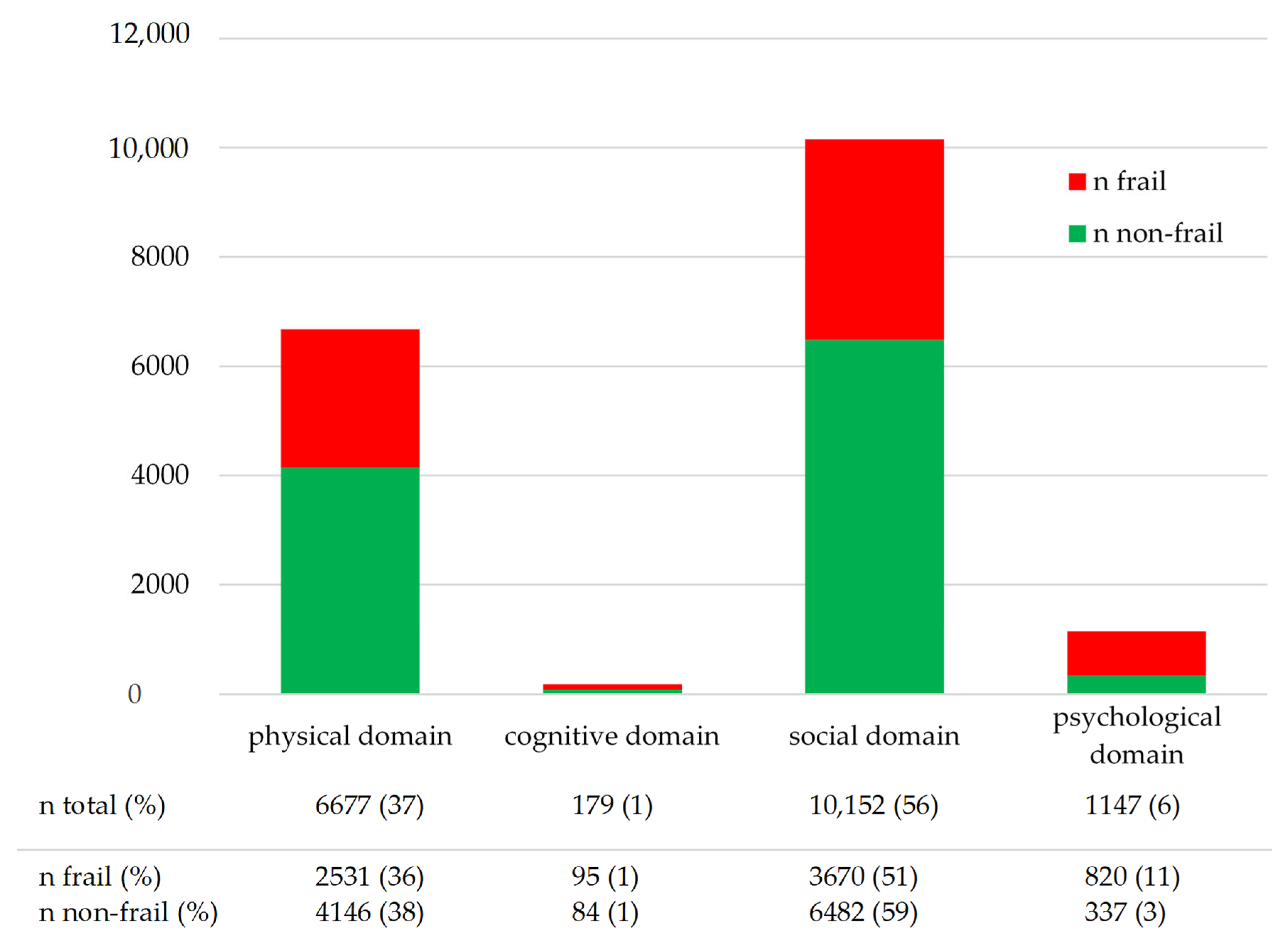
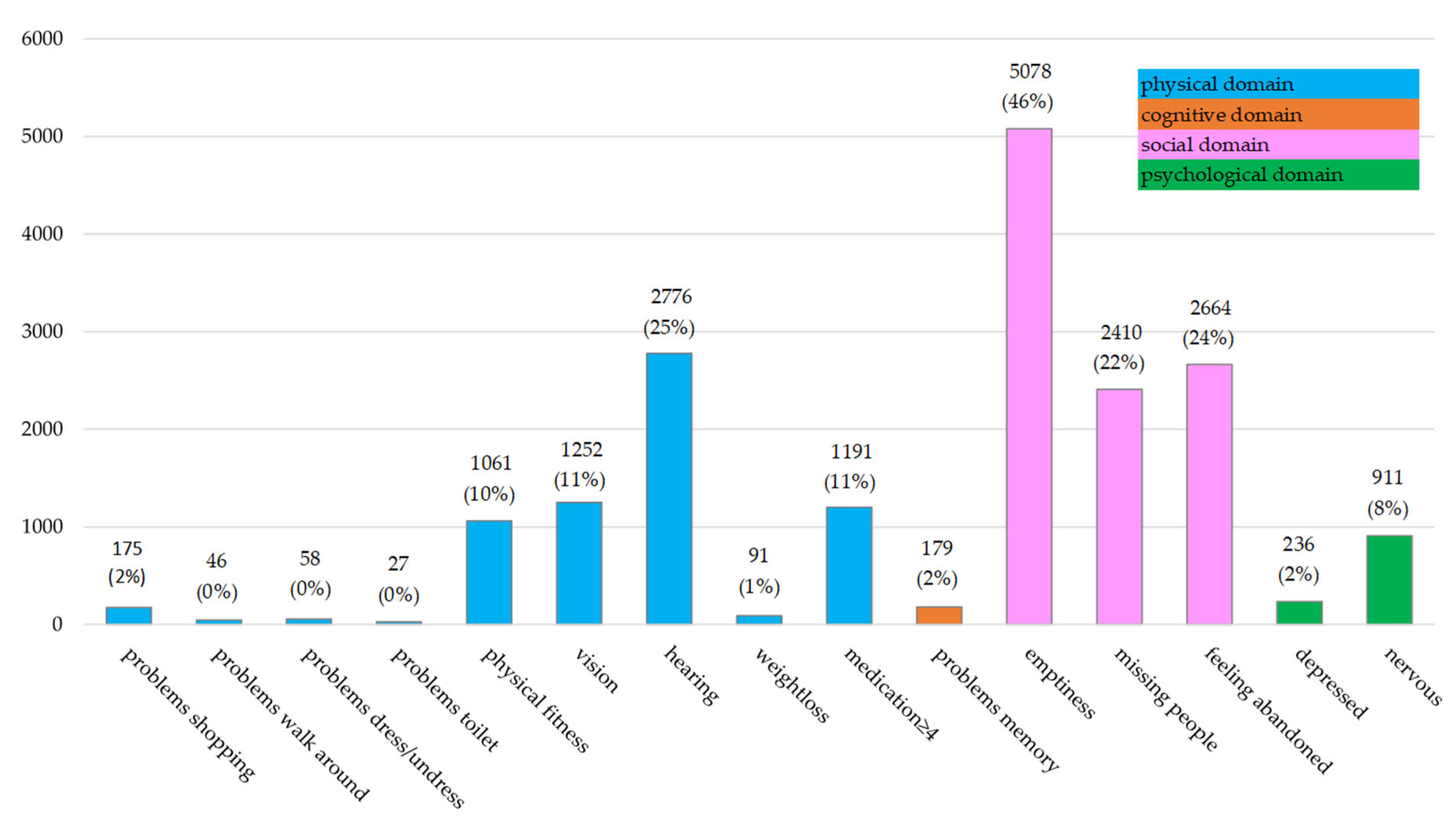
3.1. Characteristics of Frailty
3.2. Examination of Concerns and Threats Resulting from the COVID-19 Pandemic in Frail versus Non-Frail People
3.3. Analyses of Variables Potentially Associated with Frailty
4. Discussion
4.1. Strengths and Limitations
4.2. Implications for Research and Practice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cullen, W.; Gulati, G.; Kelly, B.D. Mental health in the COVID-19 pandemic. QJM Int. J. Med. 2020, 113, 311–312. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.; Singh, J. COVID-19 and its impact on society. Electron. Res. J. Soc. Sci. Humanit. 2020, 2. Available online: https://ssrn.com/abstract=3567837 (accessed on 3 March 2022).
- Boccardi, V.; Ruggiero, C.; Mecocci, P. COVID-19: A Geriatric Emergency. Geriatrics 2020, 5, 24. [Google Scholar] [CrossRef]
- Liu, K.; Chen, Y.; Lin, R.; Han, K. Clinical features of COVID-19 in elderly patients: A comparison with young and middle-aged patients. J. Infect. 2020, 80, e14–e18. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, N.E.; Wallick, A.; Brown, L.M. Impact of COVID-19 pandemic restrictions on community-dwelling caregivers and persons with dementia. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, S220. [Google Scholar] [CrossRef] [PubMed]
- Gobbens, R.J.; Luijkx, K.G.; Wijnen-Sponselee, M.T.; Schols, J.M. Toward a conceptual definition of frail community dwelling older people. Nurs. Outlook 2010, 58, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Hogan, D.B. Models, definitions, and criteria for frailty. In Conn’s Handbook of Models for Human Aging; Academic Press: Cambridge, MA, USA, 2018; pp. 35–44. [Google Scholar]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G. Frailty in older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef]
- Karunananthan, S.; Wolfson, C.; Bergman, H.; Béland, F.; Hogan, D.B. A multidisciplinary systematic literature review on frailty: Overview of the methodology used by the Canadian Initiative on Frailty and Aging. BMC Med. Res. Methodol. 2009, 9, 68. [Google Scholar] [CrossRef] [PubMed]
- Campbell, A.J.; Buchner, D.M. Unstable disability and the fluctuations of frailty. Age Ageing 1997, 26, 315–318. [Google Scholar] [CrossRef]
- Bortz, W.M. A conceptual framework of frailty: A review. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2002, 57, M283–M288. [Google Scholar] [CrossRef] [PubMed]
- Hoogendijk, E.O.; Afilalo, J.; Ensrud, K.E.; Kowal, P.; Onder, G.; Fried, L.P. Frailty: Implications for clinical practice and public health. Lancet 2019, 394, 1365–1375. [Google Scholar] [CrossRef]
- Fulop, T.; Larbi, A.; Witkowski, J.M.; McElhaney, J.; Loeb, M.; Mitnitski, A.; Pawelec, G. Aging, frailty and age-related diseases. Biogerontology 2010, 11, 547–563. [Google Scholar] [CrossRef]
- Kojima, G.; Liljas, A.E.M.; Iliffe, S. Frailty syndrome: Implications and challenges for health care policy. Risk Manag. Healthc. Policy. 2019, 12, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Sandini, M.; Pinotti, E.; Persico, I.; Picone, D.; Bellelli, G.; Gianotti, L. Systematic review and meta-analysis of frailty as a predictor of morbidity and mortality after major abdominal surgery. BJS Open 2017, 1, 128–137. [Google Scholar] [CrossRef]
- Peters, L.L.; Burgerhof, J.G.; Boter, H.; Wild, B.; Buskens, E.; Slaets, J.P. Predictive validity of a frailty measure (GFI) and a case complexity measure (IM-E-SA) on healthcare costs in an elderly population. J. Psychosom. Res. 2015, 79, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Mc Intyre, K.; Lanting, P.; Deelen, P.; Wiersma, H.; Vonk, J.M.; Ori, A.P.; Jankipersadsing, S.A.; Warmerdam, R.; van Blokland, I.; Boulogne, F. The Lifelines COVID-19 Cohort: A questionnaire-based study to investigate COVID-19 infection and its health and societal impacts in a Dutch population-based cohort. BMJ Open 2021, 11, e044474. [Google Scholar] [CrossRef]
- Rijksoverheid Maatregelen Corona Verlengd. Available online: https://www.rijksoverheid.nl/actueel/nieuws/2020/04/21/maatregelen-corona-verlengd (accessed on 29 January 2021).
- de Haas, M.; Faber, R.; Hamersma, M. How COVID-19 and the Dutch ‘intelligent lockdown’change activities, work and travel behaviour: Evidence from longitudinal data in The Netherlands. Transp. Res. Interdiscip. Perspect. 2020, 6, 100150. [Google Scholar]
- Hale, T.; Angrist, N.; Hale, A.J.; Kira, B.; Majumdar, S.; Petherick, A.; Phillips, T.; Sridhar, D.; Thompson, R.N.; Webster, S. Government responses and COVID-19 deaths: Global evidence across multiple pandemic waves. PLoS ONE 2021, 16, e0253116. [Google Scholar] [CrossRef] [PubMed]
- Scholtens, S.; Smidt, N.; Swertz, M.A.; Bakker, S.J.; Dotinga, A.; Vonk, J.M.; Van Dijk, F.; van Zon, S.K.; Wijmenga, C.; Wolffenbuttel, B.H. Cohort Profile: LifeLines, a three-generation cohort study and biobank. Int. J. Epidemiol. 2015, 44, 1172–1180. [Google Scholar] [CrossRef]
- Eurostat, the Statistical Office of the European Union ICT Usage in Households and by Individuals (isoc_i), Households—Level of Internet Access. Available online: https://ec.europa.eu/eurostat/cache/metadata/en/isoc_i_esms.htm (accessed on 3 March 2022).
- Klijs, B.; Scholtens, S.; Mandemakers, J.J.; Snieder, H.; Stolk, R.P.; Smidt, N. Representativeness of the LifeLines cohort study. PLoS ONE 2015, 10, e0137203. [Google Scholar] [CrossRef]
- Schuurmans, H.; Steverink, N.; Lindenberg, S.; Frieswijk, N.; Slaets, J.P. Old or frail: What tells us more? J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2004, 59, M962–M965. [Google Scholar] [CrossRef]
- Aaldriks, A.A.; Maartense, E.; Le Cessie, S.; Giltay, E.J.; Verlaan, H.; Van der Geest, L.; Kloosterman-Boele, W.M.; Peters-Dijkshoorn, M.T.; Blansjaar, B.A.; Van Schaick, H.W. Predictive value of geriatric assessment for patients older than 70 years, treated with chemotherapy. Crit. Rev. Oncol. 2011, 79, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Peters, L.L.; Boter, H.; Burgerhof, J.G.; Slaets, J.P.; Buskens, E. Construct validity of the Groningen Frailty Indicator established in a large sample of home-dwelling elderly persons: Evidence of stability across age and gender. Exp. Gerontol. 2015, 69, 129–141. [Google Scholar] [CrossRef] [PubMed]
- Centraal Bureau Statistiek Kerncijfers per Postcode. Available online: https://www.cbs.nl/nl-nl/dossier/nederland-regionaal/geografische-data/gegevens-per-postcode (accessed on 9 December 2020).
- Sociaal Cultureel Planbureau Sociaal Economische Status per Postcode Gebied. Available online: https://bronnen.zorggegevens.nl/Bron?naam=Sociaal-Economische-Status-per-postcodegebied (accessed on 9 December 2020).
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Derogatis, L.R.; Lipman, R.S.; Covi, L. SCL-90. Administration, Scoring and Procedures Manual-I for the R (Revised) Version and Other Instruments of the Psychopathology Rating Scales Series; Johns Hopkins University School of Medicine: Chicago, IL, USA, 1977. [Google Scholar]
- Health Council of The Netherlands. Physical activity and risk of chronic diseases. In Backgroud Document to the Dutch Physical Activity Guidelines 2017; Health Council of The Netherlands: The Hague, The Netherlands, 2017; publication no. 2017/08B. [Google Scholar]
- Helliwell, J.F.; Huang, H.; Wang, S.; Norton, M. Statistical Appendix for Chapter 2 of World Happiness Report 2020; Sustainable Development Solutions Network: New York, NY, USA, 2020. [Google Scholar]
- Drubbel, I.; Numans, M.E.; Kranenburg, G.; Bleijenberg, N.; de Wit, N.J.; Schuurmans, M.J. Screening for frailty in primary care: A systematic review of the psychometric properties of the frailty index in community-dwelling older people. BMC Geriatr. 2014, 14, 27. [Google Scholar] [CrossRef] [PubMed]
- Gobbens, R.J.; Krans, A.; van Assen, M.A. Validation of an integral conceptual model of frailty in older residents of assisted living facilities. Arch. Gerontol. Geriatr. 2015, 61, 400–410. [Google Scholar] [CrossRef] [PubMed]
- Derogatis, L.R.; Cleary, P.A. Confirmation of the dimensional structure of the SCL-90: A study in construct validation. J. Clin. Psychol. 1977, 33, 981–989. [Google Scholar] [CrossRef]
- Zhang, X.; Tan, S.S.; Franse, C.B.; Alhambra-Borrás, T.; Durá-Ferrandis, E.; Bilajac, L.; Markaki, A.; Verma, A.; Mattace-Raso, F.; Voorham, A.J. Association between physical, psychological and social frailty and health-related quality of life among older people. Eur. J. Public Health 2019, 29, 936–942. [Google Scholar] [CrossRef]
- Gobbens, R.J.; van Assen, M.A. Associations between multidimensional frailty and quality of life among Dutch older people. Arch. Gerontol. Geriatr. 2017, 73, 69–76. [Google Scholar] [CrossRef]
- Vektis Factsheet Kwetsbare Ouderen. Available online: https://www.vektis.nl/intelligence/publicaties/factsheet-kwetsbare-ouderen#:~:text=In%20alle%20leeftijdsgroepen%20is%20het,en%2045%25%20van%20de%20vrouwen (accessed on 21 February 2021).
- Collard, R.M.; Boter, H.; Schoevers, R.A.; Oude Voshaar, R.C. Prevalence of frailty in community-dwelling older persons: A systematic review. J. Am. Geriatr. Soc. 2012, 60, 1487–1492. [Google Scholar] [CrossRef]
- Gordon, E.H.; Peel, N.M.; Samanta, M.; Theou, O.; Howlett, S.E.; Hubbard, R.E. Sex differences in frailty: A systematic review and meta-analysis. Exp. Gerontol. 2017, 89, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Franse, C.B.; van Grieken, A.; Qin, L.; Melis, R.J.; Rietjens, J.A.; Raat, H. Socioeconomic inequalities in frailty and frailty components among community-dwelling older citizens. PLoS ONE 2017, 12, e0187946. [Google Scholar] [CrossRef] [PubMed]
- Hoogendijk, E.O.; van Hout, H.P.; Heymans, M.W.; van der Horst, H.E.; Frijters, D.H.; van Groenou, M.I.B.; Deeg, D.J.; Huisman, M. Explaining the association between educational level and frailty in older adults: Results from a 13-year longitudinal study in The Netherlands. Ann. Epidemiol. 2014, 24, 538–544.e2. [Google Scholar] [CrossRef] [PubMed]
- Bunt, S.; Steverink, N.; Olthof, J.; Van Der Schans, C.P.; Hobbelen, J. Social frailty in older adults: A scoping review. Eur. J. Ageing 2017, 14, 323–334. [Google Scholar] [CrossRef] [PubMed]
- Boreskie, K.F.; Hay, J.L.; Duhamel, T.A. Preventing Frailty Progression during the COVID-19 Pandemic. J. Frailty Aging 2020, 9, 130–131. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total (n = 11,145) | Frail (n = 1463; 13%) | Non-Frail (n = 9682; 87%) | ||
|---|---|---|---|---|
| Groningen Frailty Indicator (GFI) | ||||
| Total GFI score (range 0–15: median [IQR]) | 1 [0–3] | 4 [4–5] | 1 [0–2] | |
| Physical domain (range 0–9; median [IQR]) | 0 [0–1] | 2 [1–2] | 0 [0–1] | |
| Cognitive domain (range 0–1; median [IQR]) | 0 [0–0 | 0 [0–0] | 0 [0–0] | |
| Social domain (range 0–3; median IQR) | 1 [0–2] | 3 [2–3] | 0 [0–1] | |
| Psychological domain (range 0–2; median [IQR]) | 0 [0–0] | 0 [0–1] | 0 [0–0] | |
| Co-variables | Difference p-value 1 | |||
| Sex: | ||||
| Male (%) | 5265 (47) | 556 (11) | 4708 (89) | <0.001 |
| Female (%) | 5880 (53) | 906 (15) | 4974 (85) | |
| Age (years; mean [SD]) | 71.1 [4.7] | 72.1 [5.3] | 71.0 [4.6] | <0.001 |
| Urbanity (n = 11,022; median [IQR])) | 0.76 [0.31–1.27] | 0.85 [0.36–1.36] | 0.75 [0.30–1.27] | <0.001 |
| Neighbourhood SES (n = 10,800; median [IQR]) | −0.65 [−1.54–0.13] | −0.75 [−1.73–0.09] | −0.62 [−1.54–0.14] | <0.001 |
| Education level (n = 10,229): | ||||
| Lower (%) | 2186 (21) | 332 (15) | 1854 (85) | |
| Medium (%) | 5077 (50) | 670 (13) | 4407 (87) | |
| Higher (%) | 2966 (29) | 346 (12) | 2620 (88) | 0.001 |
| Single household (n = 11,142; (%)) | 1955 (18) | 434 (22) | 1521 (78) | <0.001 |
| Quality of life (n = 11,070): satisfaction > average (score > 7.5 (%)) | 5991 (53) | 261 (4) | 5561 (96) | <0.001 |
| Charlson co-morbidity index (n = 10,637); median [IQR] | 0 [0–1] | 1 [0–2] | 0 [0–1] | <0.001 |
| Satisfaction with social support: (satisfied (%)) | 7835 (70) | 989 (13) | 6846 (87) | 0.015 |
| Physical discomfort score of past 7 days (n = 10,894); median [IQR] | 13 [12–15] | 15 [13–18] | 13 [12–15] | <0.001 |
| Problems sleeping almost every night (n = 11,144; yes (%)) | 1496 (13) | 501 (34) | 995 (66) | <0.001 |
| Change in appetite or body weight (yes (%)) | 364 (3) | 146 (40) | 218 (60) | <0.001 |
| Self-reported moderately inthensive physical activity >150 min/week (n = 11,133; no (%)) | 4332 (39) | 787 (18) | 3545 (82) | <0.001 |
| Alcohol (n = 11,101; glass p/week; median [IQR]) | 2 [0–7] | 1 [0–5] | 3 [0–7] | <0.001 |
| Smoking in the last week (n = 11,144; yes (%)) | 470 (4) | 84 (18) | 386 (82) | 0.002 |
| Item | Answer | Frail n (%) | Non-Frail n (%) | p-Value Chi2 Test |
|---|---|---|---|---|
| How much have you been concerned about the COVID-19 pandemic in the past 7 days (n = 9589)? | 1 not worried | 33 (3) | 855 (10) * | <0.001 |
| 2 | 62 (5) | 1466 (18) * | ||
| 3 | 90 (7) | 1361 (16) * | ||
| 4 | 82 (7) | 764 (9) * | ||
| 5 | 211 (17) * | 1139 (14) | ||
| 6 | 219 (18) * | 1106 (14) | ||
| 7 | 298 (24) * | 1137 (14) | ||
| 8 | 170 (14) * | 467 (6) | ||
| 9–10 severely worried | 57 (5) * | 72 (1) | ||
| Total | 1222 (100) | 8367 (100) | ||
| I worry about getting sick myself (n = 11,069). | Never | 89 (6) | 1608 (17) * | <0.001 |
| Almost never | 359 (25) | 4129 (43) * | ||
| Sometimes | 767 (53) * | 3549 (37) | ||
| Often | 210 (14) * | 287 (3) | ||
| (Almost) Always | 30 (2) * | 41 (0) | ||
| Total | 1455 (100) | 9614 (100) | ||
| I worry that someone close to me will get sick (n = 11,069). | Never | 76 (5) | 1233 (13) * | <0.001 |
| Almost never | 247 (17) | 3164 (33) * | ||
| Sometimes | 763 (52) * | 4487 (47) | ||
| Often | 310 (21) * | 654 (7) | ||
| (Almost) Always | 59 (4) * | 76 (1) | ||
| Total | 1455 (100) | 9614 (100) | ||
| I am concerned that I or my family will be in serious financial trouble (n = 11,063). | Never | 543 (37) | 5378 (56) * | <0.001 |
| Almost never | 384 (26) | 2708 (28) | ||
| Sometimes | 413 (28) * | 1364 (14) | ||
| Often | 99 (7) * | 140 (2) | ||
| (Almost) Always | 17 (1) * | 17 (0) | ||
| Total | 1456 (100) | 9607 (100) | ||
| I worry that it will be a long time before my life returns to normal n = 11,048). | Never | 113 (8) | 2199 (23) * | <0.001 |
| Almost never | 159 (11) | 2606 (27) * | ||
| Sometimes | 668 (46) * | 3844 (40) | ||
| Often | 434 (30) * | 884 (9) | ||
| (Almost) Always | 78 (5) * | 63 (1) | ||
| Total | 1452 (100) | 9596 (100) | ||
| I am concerned that I can’t see friends and family n = 11,060). | Never | 75 (5) | 1616 (17) * | <0.001 |
| Almost never | 167 (12) | 2748 (29) * | ||
| Sometimes | 644 (44) | 4146 (43) | ||
| Often | 481 (33) * | 1028 (11) | ||
| (Almost) Always | 86 (6) * | 67 (1) | ||
| Total | 1453 (100) | 9605 (100) | ||
| The Coronavirus threatens everyone in The Netherlands (n = 11,067). | Totally disagree | 31 (2) | 210 (2) | <0.001 |
| Disagree slightly | 29 (2) | 329 (3) * | ||
| Neutral | 55 (4) | 486 (5) * | ||
| Agree slightly | 311 (21) | 2434 (25) * | ||
| Totally agree | 1032 (71) * | 6150 (64) | ||
| Total | 1458 (100) | 9609 (100) | ||
| Since the beginning of the COVID-19 pandemic, I see others in my area, such as people in the neighborhood or in shops, as a threat to my well-being (n = 11.061). | Totally disagree | 86 (6) | 1230 (13) * | <0.001 |
| Disagree slightly | 134 (9) | 1389 (14) * | ||
| Neutral | 187 (13) | 1358 (14) | ||
| Agree slightly | 791 (54) * | 4740 (49) | ||
| Totally agree | 257 (18) * | 889 (9) | ||
| Total | 1455 (100) | 9606 (100) |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| Variables | p-Value | OR (95% CI) | p-Value | OR (95% CI) |
| Sex (female) | <0.001 | 1.54 (1.38–1.72) | 0.168 | 1.11 (0.96–1.29) |
| Age (years) | <0.001 | 1.05 (1.04–1.06) | <0.001 | 1.04 (1.03–1.06) |
| Urbanity | <0.001 | 1.13 (1.08–1.19) | 0.225 | 1.04 (0.97–1.12) |
| Neighborhood SES | 0.002 | 0.91 (0.87–0.96) | 0.235 | 0.97 (0.91–1.02) |
| Education level (low vs. middle, low vs. high) | 0.003 0.136 | 1.36 (1.15–1.60) 1.15 (1.00–1.32) | 0.325 0.708 | 1.11 (0.91–1.35) 0.97 (0.82–1.14) |
| Single household (yes) | <0.001 | 2.27 (2.00–2.57) | <0.001 | 1.81 (1.54–2.13) |
| Quality of life (>7.5) | <0.001 | 0.16 (0.14–0.19) | <0.001 | 0.23 (0.19–0.27) |
| Charlson co-morbidity index | <0.001 | 1.57 (1.49–1.65) | <0.001 | 1.23 (1.16–1.30) |
| Social support (satisfied) | 0.041 | 0.86 (0.77–0.97) | 0.284 | 0.92 (0.80–1.07) |
| Physical discomfort score of the past 7 days | <0.001 | 1.30 (1.28–1.32) | <0.001 | 1.19 (1.16–1.21) |
| Problems sleeping almost every night (yes) | <0.001 | 4.55 (4.01–5.17) | <0.001 | 1.98 (1.67–2.33) |
| Change in appetite or body weight (yes) | <0.001 | 4.81 (3.87–5.98) | <0.001 | 1.89 (1.41–2.54) |
| Moderately intensive physical activity > 150 min/week (yes) | <0.001 | 0.50 (0.44–0.55) | <0.001 | 0.76 (0.66–0.87) |
| Alcohol (n glasses/week) | <0.001 | 0.97 (0.96–0.98) | 0.110 | 0.99 (0.98–1.00) |
| Smoking last week (yes) | <0.001 | 1.47 (1.15–1.87) | 0.018 | 1.45 (1.07–1.99) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sealy, M.J.; van der Lucht, F.; van Munster, B.C.; Krijnen, W.P.; Hobbelen, H.; Barf, H.A.; Finnema, E.J.; Jager-Wittenaar, H. Frailty among Older People during the First Wave of the COVID-19 Pandemic in The Netherlands. Int. J. Environ. Res. Public Health 2022, 19, 3669. https://doi.org/10.3390/ijerph19063669
Sealy MJ, van der Lucht F, van Munster BC, Krijnen WP, Hobbelen H, Barf HA, Finnema EJ, Jager-Wittenaar H. Frailty among Older People during the First Wave of the COVID-19 Pandemic in The Netherlands. International Journal of Environmental Research and Public Health. 2022; 19(6):3669. https://doi.org/10.3390/ijerph19063669
Chicago/Turabian StyleSealy, Martine J., Fons van der Lucht, Barbara C. van Munster, Wim P. Krijnen, Hans Hobbelen, Hans A. Barf, Evelyn J. Finnema, and Harriët Jager-Wittenaar. 2022. "Frailty among Older People during the First Wave of the COVID-19 Pandemic in The Netherlands" International Journal of Environmental Research and Public Health 19, no. 6: 3669. https://doi.org/10.3390/ijerph19063669