
Sustainable Return to Work for Workers with Mental Health and Musculoskeletal Conditions

Abstract
:1. Introduction
2. Materials and Methods
2.1. Recruitment
2.2. Realist Evaluation Phase
2.2.1. Phase 1–Theory Gleaning
Data Collection
2.2.2. Phase 2–Theory Refining or Creation
Data Analysis
2.2.3. Phase 3–Theory Consolidation
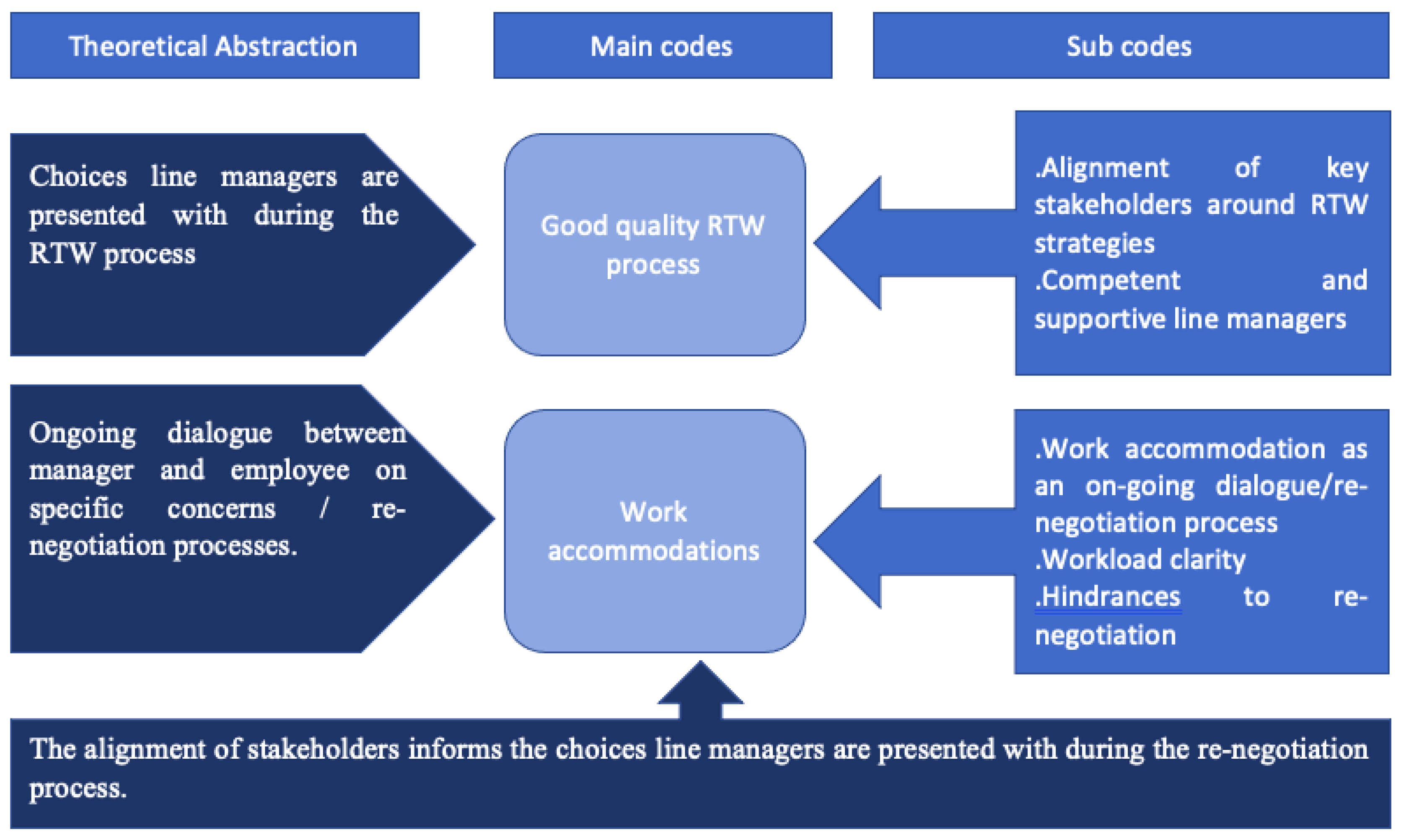
3. Results
- Choices presented to line managers during the RTW process.
- Ongoing dialogue between manager and employee on specific concerns/re-negotiation processes.
- The alignment of stakeholders informs the choices presented to line managers during the re-negotiation process.
3.1. Choices Presented to Line Managers during the RTW Process
3.1.1. Good Quality RTW Process
The Alignment of Key Stakeholders around RTW Strategy
“When I came back, we had a return-to-work interview which went ok… Ok, so, I started with low level of cases and I had phased return that was suggested by Occupational Health”(015-F-40+)
“It was me feeling confident that the manager understood me as a person and understood my condition… I think it helped them understand better what support they needed to put in place.”(022-M-40+)
“….if I say, ‘my back’s bad, driving is typical, can we consider the working from home because let’s face it, you haven’t even answered me from January’ (Laughing). It will be… I will ask the service management and then I’m pretty certain the answer will be NO! So, it is kind of blocked. So, the line manager is lovely, she’ll listen to you, but they are very restricted in what they can do to help. So, 9 out of 10 times it’s blocked.”(002-F-30+)
Competent and Supportive Line Manager
“…The manager who I was working with at the time during my return was far better equipped to deal with people in my position and people with some mental health issues. The manager back where I was in my substantive role had absolutely zero ability in my opinion and I think others as well deal with that kind of situation.”(022-M-40+)
3.2. Ongoing Dialogue between Manager and Employee on Specific Concerns/Re-Negotiation Processes
3.2.1. Work Accommodation
Work Accommodation as an On-Going Dialogue/Re-Negotiation Process
“So, I came back, worked here and that didn’t work terribly well and then they said you could work from home for a few days. That really helped until I could sort out how to get to work better.”(014-F-40+, MSDs & 2 weeks absence)
“I think what was helpful was the fact that I could work shorter hours and I got to choose them. And what I mean by that was I was offered…. You know, if I was going for half a day, would I prefer to do the morning, or would I prefer to do the afternoon. Because some... for me I chose the mornings because I get up and do the school runs anyways and I found that come the afternoon I was sore… So, for me that was really helpful.”(012-F-30+, MSDs & 6 weeks absence)
“I was phased on 25% for …. I can’t really remember a 100%. 25% was for two or three weeks, and then it was 50% for about two or three weeks and then it went to 75% for a week and then full time. So, it was needed another block between 75 and 100% if that makes sense. Because that feels like a very big step, from 75% to 100. It’s not because it’s no bigger than the other steps, but it’s just when you’re coming back it feels like a big jump.”(005-F-40+)
“… It was occupational health who were obviously involved and then the colleagues that’s just sort of a subcontracted situation. But they, if I recall correctly, they… I went and spoke to them a couple of times and they made recommendations around the phase return and then my manager then took that on board. It was phased in terms of numbers of days of the week. And also, I went and worked for a different Department for a while, so that I was able to sort of break myself back into the grass roots of things because there was an awful lot of changes going on. So, it was quite important that I started to pick up on what was required and how the role had shifted.”(009-M-40+)
“I think I was off for six or seven months, so to come back in a couple of days a week to start off with you know, … I think it was a couple of days a week to start off with, and then that built over say six weeks back up to a full full-time role. It was… it made life easy… how can I describe? It meant that I didn’t feel that I was under immediate pressure to perform, to take on board everything that was going on.”(009-M-40+, CMD & 7 months)
Workload Clarity
“…it could be better simply by better communication and getting a clearer picture of what somebody can do when they come back rather than you go to occupational health, they say phased return, so your manager sits down with you and you work out the pattern of phased return and then off you go. Whereas, when you’re sitting down and talking about the phased return it needs to include ‘how are you emotionally, and physically what can you do?...”(016-F-40+)
“… I suppose it’s that reassurance and almost reiteration of it. It’s very easy to just go ‘its ok, you can do this’ and then never mention it again. So, I think that repetition of ‘it’s still ok, this is ok, I accept that, this isn’t getting done but that’s ok’. But I think probably what I didn’t do with my manager was sit down and look at the work that I’ve got on because they probably don’t know the work that I’ve got, and they trust me to do that...”(020-M-40+)
“I think they were probably a bit surprised that I came in to work with my arm in a sling and tried to work (laughing). They kept on saying to me ‘are you sure you should be at work?’ And you know, ‘can you manage?’ And I thought I could manage. And I remember telling you this and then I realised that no, you know I couldn’t drive, and I had to walk back to the station with a laptop and another bag. And I just realised that I couldn’t do that on a daily basis because it was exhausting when you’re struggling the whole time and so then they said that I could work from home and that was what made a … that made a big difference.”(014-F-40+)
Hindrances to Re-Negotiation
“But being not so integrated in the team that is something I just accept that. I find it sometimes painful, allowing me feel what I feel, but I feel like I can’t change it really…”(015-F-40+, CMDs)
“.... The flip side of that is this glass ceiling and you’re perceived to be a bit flaky. So how do you minimise that? Because you’ve had a bleep (mental break-down), that you’re a bit flaky and that you can’t do your job.”(011-F-40+, CMDs)
“It’s difficult because as I said then, going back to this previous line manager and you know after I got back last time and then dealing with this person who I could have put in a complaint with. So, it’s basically being line-managed by the person who was the problem and so I suppose it was an unusual case in that respect.”(019-M-30+, CMDs)
“In my experience with what I’ve had, it was very good. I think that it’s unique to me. I’m almost thankful for what I’ve got because I recognise that this isn’t standard and I don’t see it elsewhere within the organisation or … it’s in places, I mean there are pockets of really good behaviours. But you see other working environments, other businesses, you know your colleague work at places, and everyone is under a lot of pressure. I don’t see this across there.”(020-M-40+, CMD/MSD)
3.3. The Alignment of Key Stakeholders Informs the Choices Line Managers Are Presented with during the On-Going Re-Negotiation Process
“…it obviously depends on what your managers have to deal with if you like, …. because they have the Occupational Health and the HR and their guidance and obviously the HR team and the Wellbeing team would have dealt with a lot more situations with people’s mental health situations. I think they’re supported by the other members of the organisation, so they are able to support you. Even if they might not understand your situation that they haven’t dealt with any mental health issues themselves, I think they’re supported enough that they can be empathetic.”(021-F-40+)
3.4. Summary of Consolidated Theories
4. Discussion
4.1. Limitations of the Study
4.2. Implications for Policy, Practice, and Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Health and Safety Executive (CMDs Report). Work-Related Stress, Anxiety or Depression Statistics in Great Britain, 2020; Health and Safety Executive: London, UK, 2020.
- Health and Safety Executive (MSDs Report). Work Related Musculoskeletal Disorder Statistics (WRMSDs) in Great Britain, 2020; Health and Safety Executive: London, UK, 2020.
- Hansmann, M.; Beller, J.; Maurer, F.; Kroger, C. Self-Efficacy Beliefs of Employees with Mental Disorders or Musculoskeletal Diseases after Sickness-Related Absence: Validation of the German Version of the Return-to-Work Self-Efficacy Scale. J. Int. Environ. Res. Public Health 2022, 19, 10093. [Google Scholar] [CrossRef] [PubMed]
- Health and Safety Executive (HSE). Mental Health Conditions, Work and the Workplace; Health and Safety Executive: London, UK, 22 May 2022. Available online: https://www.hse.gov.uk/stress/mental-health.htm (accessed on 15 December 2022).
- World Health Organisation. Musculoskeletal Health; World Health Organisation: Geneva, Switzerland, 14 July 2022; Available online: https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions (accessed on 15 December 2022).
- Etuknwa, A.; Daniels, K.; Eib, C. Sustainable Return to Work: A Systematic Review Focusing on Personal and Social Factors. J. Occup. Rehabil. 2019, 29, 679–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lallukka, T.; Hiilamo, A.; Oakman, J.; Manty, M.; Pietilainen, O.; Rahkonen, O.; Kouvonen, A.; Halonen, J.I. Recurrent pain and work disability: A record linkage study. Int. Arch. Occup. Environ. Health 2020, 93, 421–432. [Google Scholar] [CrossRef] [Green Version]
- Gaspar, F.W.; Zaidel, C.S.; Dewa, C.S. Rates and predictors of recurrent work disability due to common mental health disorders in the United States. PLoS ONE 2018, 13, e0205170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altiraifi, A. Advancing Economic Security for People with Disabilities. 26 July 2019. Available online: https://www.americanprogress.org/issues/disability/reports/2019/07/26/472686/advancing-economic-security-people-disabilities/ (accessed on 21 May 2021).
- World Health Organisation. 10 Facts on Disability. 2017. Available online: https://www.who.int/features/factfiles/disability/en/ (accessed on 21 May 2021).
- Health and Safety Executive (HSE). Health and Safety at Work Summary Statistics for Great Britain 2022; Health and Safety Executive/National Statistics: London, UK, 2022.
- Health and Safety Executive (HSE). Health and Safety at Work Summary Statistics for Great Britain 2021; Health and Safety Executive and National Statistics: London, UK, 2021.
- Roelen, C.M.; Koopmans, P.C.; Groothoff, J.W.; van der Klink, J.L.; Bultmann, U. Return to Work After Cancer Diagnosed in 2002, 2005 and 2008. J. Occup. Rehabil. 2011, 21, 335–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, F.; Haslam, C.; Munir, F.; Pryce, J. Returning to work following cancer: A qualitative exploratory study into the experience of returning to work following cancer. Eur. J. Cancer Care 2007, 16, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Branicki, L.; Kalfa, S.; Brammer, S. Conceptualizing Responsible Return to Work: Corporate Social Responsibility in Relation to Employee Return to Work after Cancer. Work. Employ. Soc. 2020, 35, 1091–1114. [Google Scholar] [CrossRef]
- Charmaz, K. Studying the Experience of Chronic Illness through Grounded Theory. In New Directions in the Sociology of Chronic and Disabling Conditions; Scambler, G., Scambler, S., Eds.; Palgrave Macmillan: London, UK, 2010; pp. 8–36. [Google Scholar]
- Munir, F.; Yarker, J.; Haslam, C. Sickness absence management: Encouraging attendance or ‘risk-taking’ presenteeism in employees with chronic illness? Disabil. Rehabil. 2008, 30, 1461–1472. [Google Scholar] [CrossRef] [Green Version]
- Walker-Bone, K.; Hollick, R. Health and work: What physicians need to know. Clin. Med. 2021, 21, 195–200. [Google Scholar] [CrossRef]
- Soklaridis, S.; Ammendolia, C.; Cassidy, D. Looking upstream to understand low back pain and return to work: Psychosocial factors as the product of system issues. Soc. Sci. Med. 2010, 71, 1557–1566. [Google Scholar] [CrossRef]
- Waddel, G.; Burton, A.K. Is work good for your health and well-being? 2006. Available online: https://cardinal-management.co.uk/wp-content/uploads/2016/04/Burton-Waddell-is-work-good-for-you.pdf (accessed on 4 December 2017).
- Corbière, M.; Mazaniello, M.; Bastien, M.-F.; Wathieu, E.; Bouchard, R.; Panaccio, A.; Guay, S.; Lecomte, T. Stakeholders’ Role and Actions in the Return-to-Work Process of Workers on Sick-Leave Due to Common Mental Disorders: A Scoping Review. J. Occup. Rehabil. 2019, 30, 381–419. [Google Scholar] [CrossRef] [PubMed]
- Cancelliere, C.; Donovan, J.; Stockkendahl, M.J.; Biscardi, M.; Ammendolia, C.; Myburgh, C.; Cassidy, D. Factors affecting return to work after injury or illness: Best evidence synthesis of systematic reviews. Chiropr. Man. Ther. 2016, 24, 1–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joosen, M.W.; Arends, I.; Lugtenberg, M.; Timmermans, J.A.; Bruijs-Schaapveld, B.C.; Terluin, B.; van Weeghel, J.; van der Klink, J.J.; Brouwers, E.P. Barriers to and Facilitators of Return to Work after Sick Leave in Workers with Common Mental Disorders: Perspectives of Workers, Mental Health Professionals, Occupational Health Professionals, General Physicians and Managers; IOSH: Wigston Leicestershire, UK, 2017. [Google Scholar]
- Young, A.; Roessler, R.; Wasiak, R.; Mcpherson, K.; van Poppel, M.M.; Anema, J.R. A developmental conceptualization of return to work. J. Occup. Rehabil. 2005, 15, 557–568. [Google Scholar] [CrossRef]
- Jetha, A.; Pransky, G.; Fish, J.; Hettinger, L.J. Return-to-Work Within a Complex and Dynamic Organizational Work Disability System. J. Occup. Rehabil. 2016, 26, 276–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikkelsen, M.B.; Rosholm, M. Systematic review and meta-analysis of interventions aimed at enhancing return to work for sick-listed workers with common mental disorders, stress-related disorders, somatoform disorders and personality disorders. Occup. Environ. Med. 2018, 75, 675–686. [Google Scholar] [CrossRef]
- Nigatu, Y.T.; Liu, Y.; Uppal, M.; McKinney, S.R.; Rao, S.; Gillis, K.; Wang, J. Intervention for enhancing return to work in individuals with a common mental illness: Systematic review and meta-analysis of randomized controlled trials. Psychol. Med. 2016, 9, 3263–3274. [Google Scholar] [CrossRef]
- Dewa, C.S.; Loong, D.; Bonato, S.; Joosen, M.C.W. The effectiveness of return to work interventions that incorporated work-focused problem-solving skills for workers with sickness absences related to mental disorders: A systematic literature review. BMJ Open 2015, 5, e007122. [Google Scholar] [CrossRef] [Green Version]
- Van Dujin, M.; Miedema, H.; Elders, L.; Burdorf, A. Barriers forearly return-to-work of workers with musculoskeletaldisorders according to occupational health physiciansand human resource managers. J. Occup. Rehabil. 2004, 14, 31–41. [Google Scholar] [CrossRef]
- Westmorland, M.G.; Williams, R. Employers and policy makerscan make a difference to the employment of persons withdisabilities. Disabil. Rehabil. 2002, 24, 802–809. [Google Scholar] [CrossRef]
- Thomas, F.; Morgan, R. Evidence-based job retention interventions for people with disabilities: A narrative literature review. J. Vocat. Rehabil. 2021, 54, 89–101. [Google Scholar] [CrossRef]
- Cullen, K.L.; Irvin, E.; Collie, A.; Clay, F.; Gensby, U.; Jennings, P.A.; Hogg-Johnson, S.; Kristman, V.; Laberge, M.; McKenzie, D.; et al. Effectiveness of Workplace Interventions in Return-to-Work for Musculoskeletal, Pain-Related and Mental Health Conditions: An Update of the Evidence and Messages for Practitioners. J. Occup. Rehabil. 2018, 28, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martimo, K.-P. Musculoskeletal Disorders, Disability and Work; Finnish Institute of Occupational Health: Helsinki, Finland, 2010. [Google Scholar]
- Viikari-Juntura, E.; Kausto, J.; Shiri, R.; Kaila-Kangas, L.; Takala, E.-P.; Karppinen, J.; Miranda, H.; Luukkonen, R.; Martimo, K.-P. Return to work after early part-time sick leave due to musculoskeletal disorders: A randomized controlled trial. Scand. J. Work. Environ. Health 2011, 38, 134–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukuoka, Y.; Dracup, K.; Takeshima, M.; Ishi, N.; Makaya, M.; Groah, L.; Kyriakidis, E. Effect of job strain and depressive symptoms upon returning to work after acute coronary syndrome. Soc. Sci. Med. 2009, 68, 1875–1881. [Google Scholar] [CrossRef]
- Steenstra, I.; Knol, D.L.; Bongers, P.M.; Anema, J.R.; van Mechelen, W.; De Vet, H. What works best for whom? An exploratory, subgroup analysis in a randomised controlled trial on the effectiveness of a workplace intervention in low back pain patients on return to work. Spine 2009, 34, 1243–1249. [Google Scholar] [CrossRef] [PubMed]
- Lydell, M.; Grahn, B.; Mansson, J.; Baigi, A.; Marklund, B. Predictive factors of sustained return to work for persons with musculoskeletal disorders who participated in rehabilitation. Work 2009, 33, 317–328. [Google Scholar] [CrossRef] [Green Version]
- Engström, L.-G.; Janson, S. Stress-related sickness absence and return to labour market in Sweden. Disabil. Rehabil. 2007, 29, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, A.; Jamal, F.; Moore, G.; Evans, R.E.; Murphy, S.; Bonell, C. Realist complex intervention science: Applying realist principles across all phases of the Medical Research Council framework for developing and evaluating complex interventions. Evaluation 2016, 22, 286–303. [Google Scholar] [CrossRef] [Green Version]
- Mirzoev, T.; Etiaba, E.; Ebenso, B.; Uzochukwu, B.; Manzano, A.; Onwujekwe, O.; Huss, R.; Ezumah, N.; Hicks, J.P.; Newell, J.; et al. Study protocol: Realist evaluation of effectiveness and sustainability of a community health workers programme in improving maternal and child health in Nigeria. Implement. Sci. 2016, 11, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Pawson, R.; Tilley, N.; Evaluation, R. Realist Evaluation, 1st ed.; Sage Publication LTD: London, UK, 1997. [Google Scholar]
- Baxter, P.; Jack, S. Qualitative Case Study Methodology: Study dedign and implementation for novice researchers. Qual. Rep. 2008, 13, 544–559. [Google Scholar] [CrossRef]
- Marchal, B.; Van Belle, S.; Westhorp, G. Realist Evaluation. 2016. Available online: https://www.betterevaluation.org/en/approach/realist_evaluation (accessed on 26 March 2020).
- Goddard, J.T. Collective Case Study. In Encyclopedia of Case Study Research; Mills, A.J., Durepos, G., Wiebe, E., Eds.; Sage Publications, Inc.: Thousands Oaks, CA, USA, 2012; pp. 164–165. [Google Scholar]
- Manzano, A. The craft of interviewing in realist evaluation. Evaluation 2016, 22, 342–360. [Google Scholar] [CrossRef]
- Doi, L.K.; Jepson, R.; Hardie, S. Realist evaluation of an enhanced health visiting. PLoS ONE 2017, 12, e0180569. [Google Scholar] [CrossRef] [Green Version]
- Mukumbang, F.C.; Marchal, B.; Van Belle, S.; Van Wyk, B. Using the realist interview approach to maintain theoretical awareness in realist studies. Qual. Res. 2020, 20, 485–515. [Google Scholar] [CrossRef] [Green Version]
- Fereday, J.; Muir-Cochrane, E. Demonstrating Rigor Using Thematic Analysis: A Hybrid Approach of Inductive and. Int. J. Qual. Methods 2006, 5, 80–92. [Google Scholar] [CrossRef]
- Kivunja, C. Distinguishing between theory, theoretical framework and conceptual framework: A systematic review of lessons from the field. Int. J. High. Educ. 2018, 7, 44–53. [Google Scholar] [CrossRef]
- Roberts, D.; Appleton, L.; Calman, L.; Large, P.; Grande, G.; Lloyd-Williams, M.; Walshe, C. Protocol for a longitudinal qualitative interview study: Maintaining psychological well-being in advanced cancer—What can we learn from patients’ and carers’ own coping strategies? BMJ Open 2013, 3, 003046. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charmaz, K. Constructing Grounded Theory; Sage: London, UK, 2006. [Google Scholar]
- Glaser, B. Basics of Grounded Theory Analysis; Sociology Press: Mill Valley, CA, USA, 1992. [Google Scholar]
- Thompson, L.; Neathey, F.; Rick, J. Best Practice in Rehabilitating Employees Following Absence Due to Work-Related Stress; HSE Books: Norwich, UK, 2003. [Google Scholar]
- Phillips, K.; Houtenville, A.; O’Neill, J.; Katz, E. The effectiveness of employer practices to recruit, hire, and retain employees with disabilities: Supervisor perspectives. J. Vocat. Rehabil. 2019, 51, 339–353. [Google Scholar] [CrossRef]
- Baril, R.; Clarke, J.; Stock, S.; Cole, D.; The Work-Ready Group. Management of return-to-work programs for workers with musculoskeletal disorders: A qualitative study in three Canadian provinces. Soc. Sci. Med. 2003, 57, 2101–2114. [Google Scholar] [CrossRef] [PubMed]
- Daniels, K.; Tregaskis, O.; Nayani, R.; Watson, D. Achieving Sustainable Workplace Wellbeing; Springer: Cham, Switzerland, 2022; In Press. [Google Scholar]
- Daniels, K.; Watson, D.; Nayani, R.; Tregaskis, O.; Hogg, M.; Etuknwa, A.; Semkina, A. Implementing practices focused on workplace health and psychological wellbeing: A systematic review. Soc. Sci. Med. 2021, 277, 113888. [Google Scholar] [CrossRef]
- Mattila-Holappa, P.; Kausto, J.; Aalto, V.; Kaila-Kangas, L.; Kivimaki, M.; Oksanen, T.; Ervasti, J. Alternative duty work as workplace-initiated procedure to reduce sickness absence. BMC Public Health 2021, 21, 1154. [Google Scholar] [CrossRef]
- Lederer, V.; Rivard, M.; Mechakra-Tahiri, S.D. Gender Differences in Personal and Work-Related Determinants of Return-to-Work Following Long-Term Disability: A 5-Year cohort study. J. Occup. Rehabil. 2012, 22, 522–531. [Google Scholar] [CrossRef]
- Chu, L.-C. Mediating toxic emotions in the workplace—The impact of abusive supervision. J. Nurs. Manag. 2014, 22, 953–963. [Google Scholar] [CrossRef] [PubMed]
- Yin, R.K. Case Study Research: Design and Methods, 4th ed.; Sage Publications: Thousand Oaks, CA, USA, 2009. [Google Scholar]
- Office of National Statistics. Sickness Absence in the UK Labour Market: February 2014; Office of National Statistics: London, UK, 2014.
- Novick, G. Is There a Bias against Telephone Interviews in Qualitative Research? Res. Nurs. Health 2008, 31, 391–398. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| CMO RTW Theories | Original Theme | |
|---|---|---|
| 1 | A competent and supportive manager, working in collaboration with other health services within the organisation (context) is likely to increase their level of understanding about employee’s condition and best RTW approach to adopt, as well as be more empathic towards employees (mechanism). As a result, they can successfully implement an effective RTW strategy (mechanism) approved by senior management, thus impacting on sustainable RTW (outcome). | Good quality RTW process |
| CMO RTW Theory | Original Theme | |
|---|---|---|
| 2 | Reassuring workers of their workload during the on-going RTW negotiation process for appropriate work accommodation(context) is effective in assuaging fear (mechanism) and assisting in easy transition back to work (outcome), which in turn impacts on successful RTW (outcome). | Workload clarity |
| CMO RTW Theory | New Theme | |
|---|---|---|
| 3 | When employees sick listed with CMD return to toxic working environments (context) during the RTW process (mechanism), it is likely to impede the negotiation process for adequate work accommodation, thereby aggravating their condition, leading to a failed RTW (outcome) | Hindrances to re-negotiation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Etuknwa, A.; Daniels, K.; Nayani, R.; Eib, C. Sustainable Return to Work for Workers with Mental Health and Musculoskeletal Conditions. Int. J. Environ. Res. Public Health 2023, 20, 1057. https://doi.org/10.3390/ijerph20021057
Etuknwa A, Daniels K, Nayani R, Eib C. Sustainable Return to Work for Workers with Mental Health and Musculoskeletal Conditions. International Journal of Environmental Research and Public Health. 2023; 20(2):1057. https://doi.org/10.3390/ijerph20021057
Chicago/Turabian StyleEtuknwa, Abasiama, Kevin Daniels, Rachel Nayani, and Constanze Eib. 2023. "Sustainable Return to Work for Workers with Mental Health and Musculoskeletal Conditions" International Journal of Environmental Research and Public Health 20, no. 2: 1057. https://doi.org/10.3390/ijerph20021057