Pipeline for Advanced Contrast Enhancement (PACE) of Chest X-ray in Evaluating COVID-19 Patients by Combining Bidimensional Empirical Mode Decomposition and Contrast Limited Adaptive Histogram Equalization (CLAHE)


 ,
,
Abstract
:1. Introduction
2. Method
3. Description and Performance Evaluation of the Algorithm
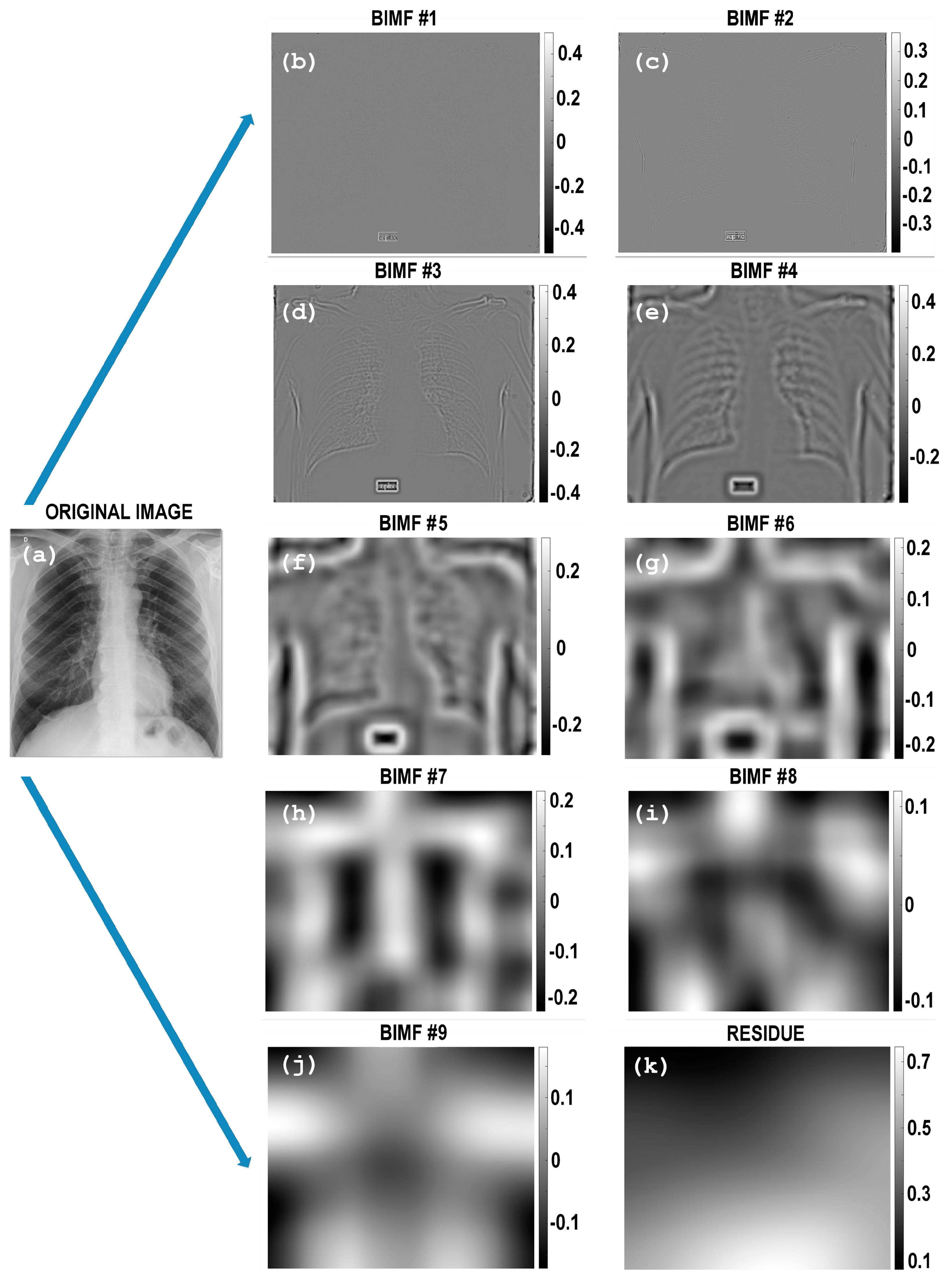
3.1. Fast and Adaptive Bidimensional Empirical Mode Decomposition—FABEMD
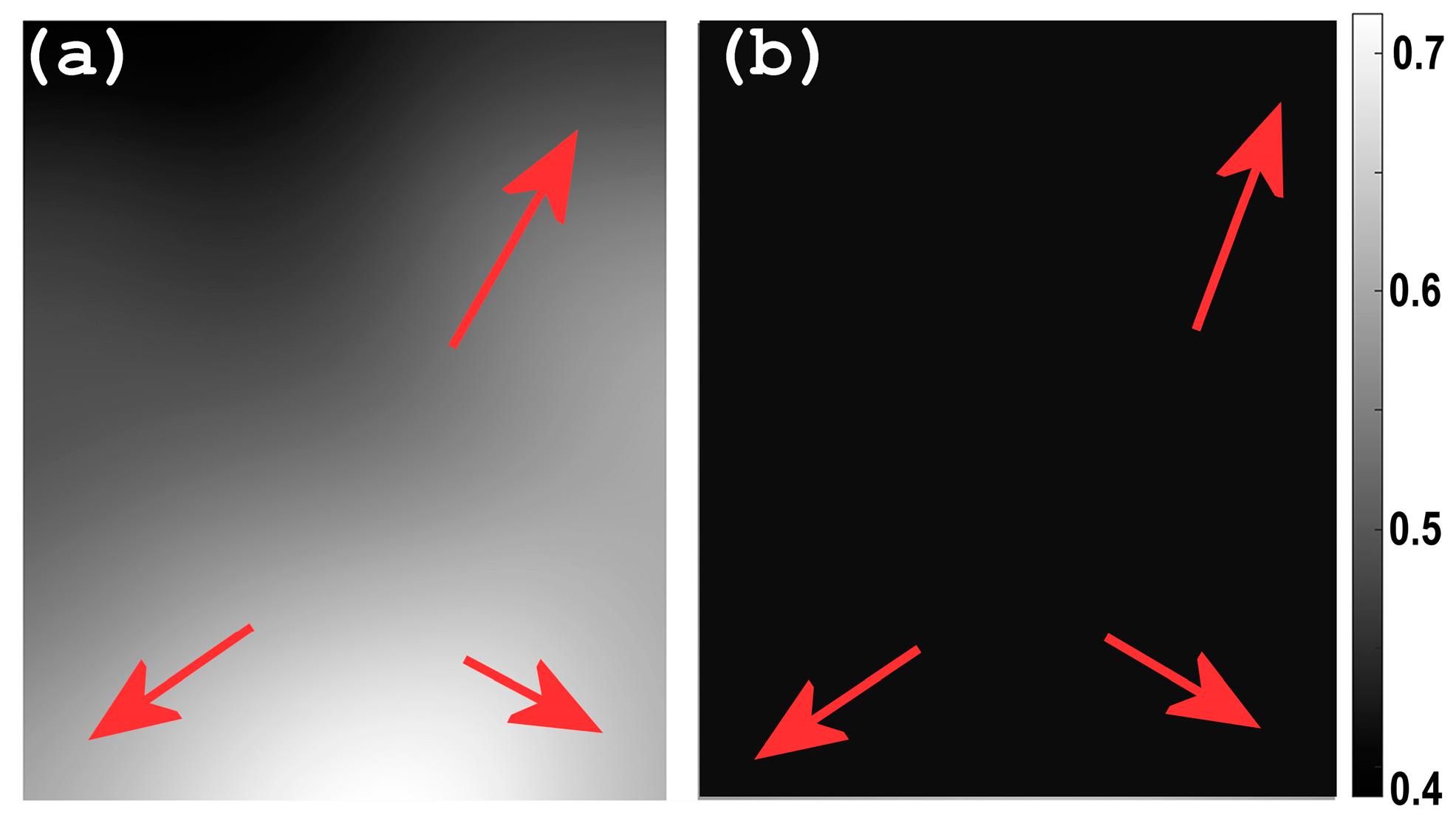
3.2. Homomorphic Filtering—HMF
3.3. Contrast Limited Adaptive Histogram Equalization—CLAHE
3.4. Metrics Definition
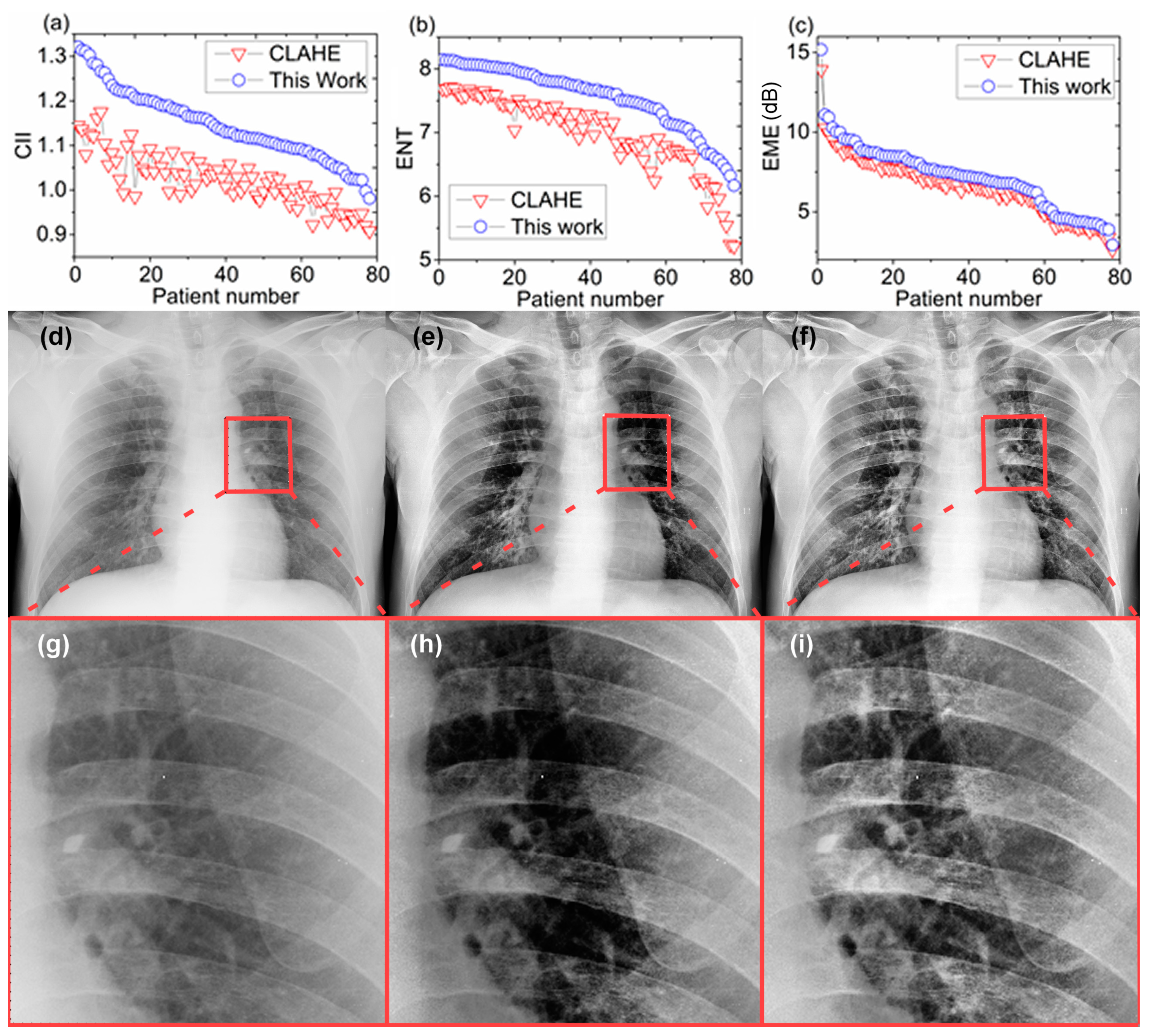
3.4.1. Contrast Improvement Index (CII)
3.4.2. Entropy—ENT
3.4.3. Measure of Enhancement—EME
4. Results and Discussion
4.1. Evaluation of the Algorithm Performance
- Adaptive Gamma Correction with Weighting Distribution (AGCWD) [74]
- Contrast Enhanced Gamma Correction (CEGAMMA) [75]
- Exposure-based Sub-Image Histogram Equalization (ESIHE) [76]
- Median-Mean-based Sub-Image Clipped Histogram Equalization (MMSICHE) [73]
- Recursive Sub-Image Exposure-based Histogram Equalization (R-ESIHE) [76]
- Dominant Orientation-based Texture Histogram Equalization (DOTHE) [72]
- Contrast Limited Adaptive Histogram Equalization (CLAHE) [38].
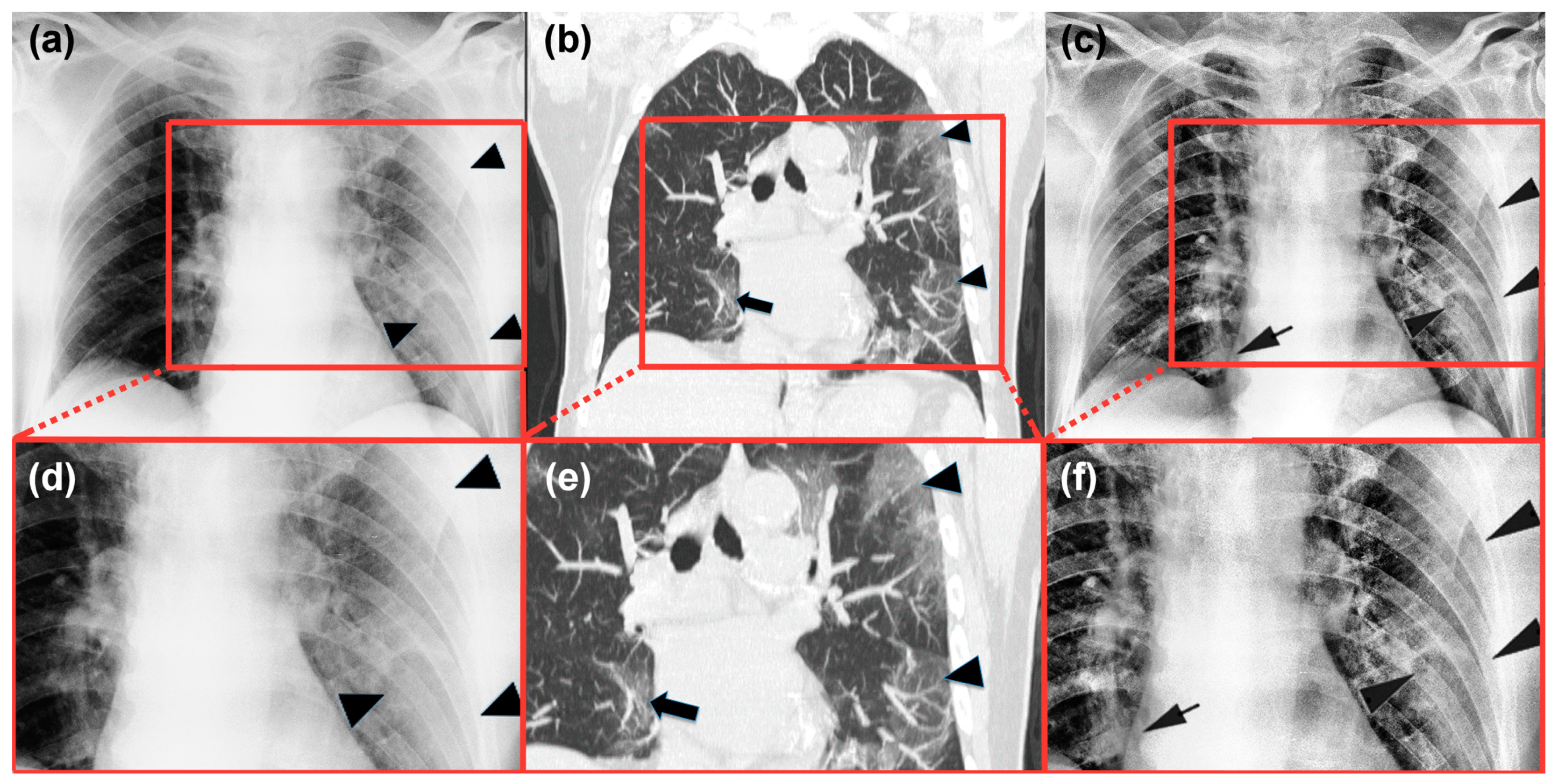
4.2. Radiological Evaluation and Statistics
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethical Statement
Data Availability
Appendix A


References
- Huda, W.; Abrahams, R.B. X-ray-based medical imaging and resolution. Am. J. Roentgenol. 2015, 204, W393–W397. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Coronavirus Disease 2019 (COVID-19) Situation Report-68; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Pan, F.; Ye, T.; Sun, P.; Gui, S.; Liang, B.; Li, L.; Zheng, D.; Wang, J.; Hesketh, R.L.; Yang, L.; et al. Time course of lung changes on chest ct during recovery from 2019 novel coronavirus (COVID-19) pneumonia. Radiology 2020, 200370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larke, F.J.; Kruger, R.L.; Cagnon, C.H.; Flynn, M.J.; McNitt-Gray, M.M.; Wu, X.; Judy, P.F.; Cody, D.D. Estimated radiation dose associated with low-dose chest ct of average-size participants in the national lung screening trial. Am. J. Roentgenol. 2011, 197, 1165–1169. [Google Scholar] [CrossRef] [PubMed]
- Mossa-Basha, M.; Meltzer, C.C.; Kim, D.C.; Tuite, M.J.; Kolli, K.P.; Tan, B.S. Radiology Department preparedness for COVID-19: Radiology scientific expert panel. Radiology 2020, 200988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, H.Y.F.; Lam, H.Y.S.; Fong, A.H.-T.; Leung, S.T.; Chin, T.W.-Y.; Lo, C.S.Y.; Lui, M.M.-S.; Lee, J.C.Y.; Chiu, K.W.-H.; Chung, T.; et al. Frequency and distribution of chest radiographic findings in COVID-19 positive patients. Radiology 2020, 201160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bandirali, M.; Sconfienza, L.M.; Serra, R.; Brembilla, R.; Albano, D.; Ernesto, P.F.; Messina, C. Chest X-ray findings in asymptomatic and minimally symptomatic quarantined patients in Codogno, Italy. Radiology 2020, 201102. [Google Scholar] [CrossRef] [Green Version]
- Ortiz-Jaramillo, B.; Kumcu, A.; Platisa, L.; Philips, W. Content-aware contrast ratio measure for images. Signal Process. Image Commun. 2018, 62, 51–63. [Google Scholar] [CrossRef]
- Qureshi, M.A.; Beghdadi, A.; Deriche, M. Towards the design of a consistent image contrast enhancement evaluation measure. Signal Process. Image Commun. 2017, 58, 212–227. [Google Scholar] [CrossRef]
- Wang, X.; Chen, L. An effective histogram modification scheme for image contrast enhancement. Signal Process. Image Commun. 2017, 58, 187–198. [Google Scholar] [CrossRef]
- Campbell, J.; Pyer, M.; Rogers, S.; Walter, D.; Reddy, R. Enabling patients with respiratory symptoms to access chest X-rays on demand: The experience of the walk-in service in Corby, UK. J. Public Health 2014, 36, 511–516. [Google Scholar] [CrossRef] [Green Version]
- Cao, A.M.Y.; Choy, J.P.; Mohanakrishnan, L.N.; Bain, R.F.; van Driel, M.L. Chest radiographs for acute lower respiratory tract infections. Cochrane Database Syst. Rev. 2013, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walz-Flannigan, A.; Magnuson, D.; Erickson, D.; Schueler, B. Artifacts in Digital Radiography. Am. J. Roentgenol. 2012, 198, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Hariri, L.P.; Mino-Kenudson, M.; Lanuti, M.; Miller, A.J.; Mark, E.J.; Suter, M.J. Diagnosing lung carcinomas with optical coherence tomography. Ann. Am. Thorac. Soc. 2015, 12, 193–201. [Google Scholar] [CrossRef] [Green Version]
- Galbois, A.; Ait-Oufella, H.; Baudel, J.-L.; Kofman, T.; Bottero, J.; Viennot, S.; Rabate, C.; Jabbouri, S.; Bouzeman, A.; Guidet, B.; et al. Pleural ultrasound compared with chest radiographic detection of pneumothorax resolution after drainage. Chest 2010, 138, 648–655. [Google Scholar] [CrossRef] [PubMed]
- Gaeta, M.; Minutoli, F.; Ascenti, G.; Vinci, S.; Mazziotti, S.; Pandolfo, I.; Blandino, A. MR white lung sign: Incidence and significance in pulmonary consolidations. J. Comput. Assist. Tomogr. 2001, 25, 890–896. [Google Scholar] [CrossRef]
- Gaeta, M.; Ascenti, G.; Mazziotti, S.; Contiguglia, R.; Barone, M.; Mileto, A. MRI differentiation of pneumonia-like mucinous adenocarcinoma and infectious pneumonia. Eur. J. Radiol. 2012, 81, 3587–3591. [Google Scholar] [CrossRef]
- Lv, D.; Qi, W.; Li, Y.; Sun, L.; Wang, Y. A cascade network for Detecting COVID-19 using chest X-rays. arXiv 2020, arXiv:2005.01468. Available online: http://arxiv.org/abs/2005.01468 (accessed on 1 May 2020).
- Tartaglione, E.; Barbano, C.A.; Berzovini, C.; Calandri, M.; Grangetto, M. Unveiling COVID-19 from Chest X-ray with deep learning: A hurdles race with small data. arXiv 2020, arXiv:2004.05405. Available online: http://arxiv.org/abs/2004.05405 (accessed on 11 April 2020).
- Oh, Y.; Park, S.; Ye, J.C. Deep learning COVID-19 features on CXR using limited training data sets. arXiv 2020, arXiv:2004.05758. Available online: http://arxiv.org/abs/2004.05758 (accessed on 5 May 2020).
- Bhuiyan, S.M.A.; Adhami, R.R.; Khan, J.F. A novel approach of fast and adaptive bidimensional empirical mode decomposition. In Proceedings of the 2008 IEEE International Conference on Acoustics, Speech and Signal Processing, Las Vegas, NV, USA, 31 March–4 April 2008; pp. 1313–1316. [Google Scholar]
- Bhuiyan, S.M.A.; Adhami, R.R.; Khan, J.F. Fast and adaptive bidimensional empirical mode decomposition using order-statistics filter based envelope estimation. EURASIP J. Adv. Signal Process. 2008, 2008, 728356. [Google Scholar] [CrossRef] [Green Version]
- Looney, D.; Mandic, D.P. Multiscale Image fusion using complex extensions of EMD. IEEE Trans. Signal Process. 2009, 57, 1626–1630. [Google Scholar] [CrossRef]
- Sotiras, A.; Davatzikos, C.; Paragios, N. Deformable medical image registration: A survey. IEEE Trans. Med. Imaging 2013, 32, 1153–1190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, W.; Xu, W.; Li, L. Medical image retrieval based on bidimensional empirical mode decomposition. In Proceedings of the 2007 IEEE 7th International Symposium on BioInformatics and BioEngineering, Boston, MA, USA, 14–17 October 2007; pp. 641–646. [Google Scholar]
- Zheng, Y.-Z.; Qin, Z. Medical image fusion algorithm based on bidimensional empirical mode decomposition. J. Softw. 2010, 20, 1096–1105. [Google Scholar] [CrossRef]
- James, A.P.; Dasarathy, B.V. Medical image fusion: A survey of the state of the art. Inf. Fusion 2014, 19, 4–19. [Google Scholar] [CrossRef] [Green Version]
- Flandrin, P.; Gonçalvès, P.; Rilling, G. EMD equivalent filter banks, from interpretation to applications. In The Hilbert-Huang Transform and Its Applications; World Scientific: Singapore, 2014; pp. 99–116. [Google Scholar]
- Pitas, I.; Venetsanopoulos, A.N. Nonlinear Digital Filters; Springer US: Boston, MA, USA, 1990; ISBN 978-1-4419-5120-5. [Google Scholar]
- Wen, H.; Qi, W.; Shuang, L. Medical X-ray image enhancement based on wavelet domain homomorphic filtering and CLAHE. In Proceedings of the 2016 International Conference on Robots & Intelligent System (ICRIS), Zhangjiajie, China, 27–28 August 2016; pp. 249–254. [Google Scholar]
- Fan, C.-N.; Zhang, F.-Y. Homomorphic filtering based illumination normalization method for face recognition. Pattern Recognit. Lett. 2011, 32, 1468–1479. [Google Scholar] [CrossRef]
- Castaño Moraga, C.A.; Westin, C.F.; Ruiz-Alzola, J. Homomorphic filtering of DT-MRI fields. In Lecture Notes in Computer Science; Springer: Berlin/Heidelberg, Germany, 2003; pp. 990–991. [Google Scholar]
- Delac, K.; Grgic, M.; Kos, T. Sub-image homomorphic filtering technique for improving facial identification under difficult illumination conditions. In Proceedings of the 13th International Conference on Systems, Signals and Image Processing, Budapest, Hungary, 21–23 September 2006. [Google Scholar]
- Dutta, P.; Saha, S. Fusion of expression values and protein interaction information using multi-objective optimization for improving gene clustering. Comput. Biol. Med. 2017, 89, 31–43. [Google Scholar] [CrossRef]
- Yang, X.-S. Multi-Objective Optimization. In Nature-Inspired Optimization Algorithms; Elsevier: Amsterdam, The Netherlands, 2014; pp. 197–211. [Google Scholar]
- Seow, M.-J.; Asari, V.K. Ratio rule and homomorphic filter for enhancement of digital colour image. Neurocomputing 2006, 69, 954–958. [Google Scholar] [CrossRef]
- Zimmerman, J.B.; Pizer, S.M.; Staab, E.V.; Perry, J.R.; McCartney, W.; Brenton, B.C. An evaluation of the effectiveness of adaptive histogram equalization for contrast enhancement. IEEE Trans. Med. Imaging 1988, 7, 304–312. [Google Scholar] [CrossRef] [Green Version]
- Zuiderveld, K. Contrast Limited Adaptive Histogram Equalization. In Graphics Gems; Elsevier: Amsterdam, The Netherlands, 1994; pp. 474–485. [Google Scholar]
- Joseph, J.; Sivaraman, J.; Periyasamy, R.; Simi, V.R. An objective method to identify optimum clip-limit and histogram specification of contrast limited adaptive histogram equalization for MR images. Biocybern. Biomed. Eng. 2017, 37, 489–497. [Google Scholar] [CrossRef]
- Al-Ameen, Z.; Sulong, G.; Rehman, A.; Al-Dhelaan, A.; Saba, T.; Al-Rodhaan, M. An innovative technique for contrast enhancement of computed tomography images using normalized gamma-corrected contrast-limited adaptive histogram equalization. EURASIP J. Adv. Signal Process. 2015, 2015, 32. [Google Scholar] [CrossRef]
- Sahu, S.; Singh, A.K.; Ghrera, S.P.; Elhoseny, M. An approach for de-noising and contrast enhancement of retinal fundus image using CLAHE. Opt. Laser Technol. 2019, 110, 87–98. [Google Scholar] [CrossRef]
- Zhou, X.; Zheng, Y.; Tan, L.; Zhao, J. Medical Image Contrast Enhancement via Wavelet Homomorphic Filtering Transform. TELKOMNIKA (Telecommun. Comput. Electron. Control.) 2016, 14, 1203. [Google Scholar] [CrossRef] [Green Version]
- Tan, Y.; Li, G.; Duan, H.; Li, C. Enhancement of medical image details via wavelet homomorphic filtering transform. J. Intell. Syst. 2014, 23, 83–94. [Google Scholar] [CrossRef]
- Panetta, K.; Zhou, Y.; Agaian, S.; Hongwei, J. Nonlinear unsharp masking for mammogram enhancement. IEEE Trans. Inf. Technol. Biomed. 2011, 15, 918–928. [Google Scholar] [CrossRef]
- Agaian, S.S.; Silver, B.; Panetta, K.A. Transform coefficient histogram-based image enhancement algorithms using contrast entropy. IEEE Trans. Image Process. 2007, 16, 741–758. [Google Scholar] [CrossRef]
- Wu, L.; Zhang, X.; Chen, H. Effective quality metric for contrast-distorted images based on SVD. Signal. Process. Image Commun. 2019, 78, 254–262. [Google Scholar] [CrossRef]
- Gonzalez, R.C.; Woods, R.E. Digital Image Processing, 3rd ed.; Pearson: London, UK, 2007; ISBN 013168728X. [Google Scholar]
- Ema, T.; Doi, K.; Nishikawa, R.M.; Jiang, Y.; Papaioannou, J. Image feature analysis and computer-aided diagnosis in mammography: Reduction of false-positive clustered microcalcifications using local edge-gradient analysis. Med. Phys. 1995, 22, 161–169. [Google Scholar] [CrossRef]
- Wu, S.; Zhu, Q.; Yang, Y.; Xie, Y. Feature and contrast enhancement of mammographic image based on multiscale analysis and morphology. In Proceedings of the 2013 IEEE International Conference on Information and Automation (ICIA), Yinchuan, China, 26–28 August 2013; pp. 521–526. [Google Scholar]
- Agaian, S.S.; Panetta, K.; Grigoryan, A.M. Transform-based image enhancement algorithms with performance measure. IEEE Trans. Image Process. 2001, 10, 367–382. [Google Scholar] [CrossRef] [Green Version]
- Kanwal, N.; Girdhar, A.; Gupta, S. Region based adaptive contrast enhancement of medical X-ray images. In Proceedings of the 2011 5th International Conference on Bioinformatics and Biomedical Engineering, Wuhan, China, 10–12 May 2011; pp. 1–5. [Google Scholar]
- Panetta, K.; Samani, A.; Agaian, S. Choosing the optimal spatial domain measure of enhancement for mammogram images. Int. J. Biomed. Imaging 2014, 2014, 1–8. [Google Scholar] [CrossRef]
- Chen, S.; Yao, L.; Chen, B. A parameterized logarithmic image processing method with Laplacian of Gaussian filtering for lung nodule enhancement in chest radiographs. Med. Biol. Eng. Comput. 2016, 54, 1793–1806. [Google Scholar] [CrossRef]
- Chen, S.; Cai, Y. Enhancement of chest radiograph in emergency intensive care unit by means of reverse anisotropic diffusion-based unsharp masking model. Diagnostics 2019, 9, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, S.; Porwal, R. Appropriate contrast enhancement measures for brain and breast cancer images. Int. J. Biomed. Imaging 2016, 2016, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sundaram, M.; Ramar, K.; Arumugam, N.; Prabin, G. Histogram modified local contrast enhancement for mammogram images. Appl. Soft Comput. 2011, 11, 5809–5816. [Google Scholar] [CrossRef]
- Arici, T.; Dikbas, S.; Altunbasak, Y. A histogram modification framework and its application for image contrast enhancement. IEEE Trans. Image Process. 2009, 18, 1921–1935. [Google Scholar] [CrossRef]
- Lee, C.; Lee, C.; Kim, C.-S. Contrast enhancement based on layered difference representation of 2D histograms. IEEE Trans. Image Process. 2013, 22, 5372–5384. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.-D. A new image quality measure for assessment of histogram equalization-based contrast enhancement techniques. Digit. Signal. Process. 2012, 22, 640–647. [Google Scholar] [CrossRef]
- Akila, K.; Jayashree, L.S.; Vasuki, A. Mammographic image enhancement using indirect contrast enhancement techniques—A comparative study. Procedia Comput. Sci. 2015, 47, 255–261. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J.P.; Morrison, P.; Dao, L. COVID-19 image data collection. arXiv 2020, arXiv:2003.11597. Available online: http://arxiv.org/abs/2003.11597 (accessed on 25 March 2020).
- Khan, S.U.; Chai, W.Y.; See, C.S.; Khan, A. X-ray image enhancement using a boundary division wiener filter and wavelet-based image fusion approach. J. Inf. Process. Syst. 2016, 12, 35–45. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y. X-ray image enhancement using the fruit fly optimization algorithm. Int. J. Simul. Syst. Sci. Technol. 2016, 2016, 44.1–44.5. [Google Scholar] [CrossRef]
- Huang, C.-C.; Nguyen, M.-H. X-ray enhancement based on component attenuation, contrast adjustment, and image fusion. IEEE Trans. Image Process. 2019, 28, 127–141. [Google Scholar] [CrossRef] [PubMed]
- Rui, W.; Guoyu, W. Medical X-ray image enhancement method based on TV-homomorphic filter. In Proceedings of the 2017 2nd International Conference on Image, Vision and Computing, ICIVC 2017, Chengdu, China, 2–4 June 2017. [Google Scholar]
- Huang, R.; Dung, L.; Chu, C. Noise removal and contrast enhancement for X-ray images. J. Biomed. Eng. Med. Imaging 2016, 3, 56. [Google Scholar] [CrossRef]
- Kim, B.; Lee, H.; Kim, K.J.; Seo, J.; Park, S.; Shin, Y.-G.; Kim, S.H.; Lee, K.H. Comparison of three image comparison methods for the visual assessment of the image fidelity of compressed computed tomography images. Med. Phys. 2011, 38, 836–844. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.P.; Krupinski, E.A.; Yan, M.; Roehrig, H.; Graham, A.R.; Weinstein, R.S. Using a visual discrimination model for the detection of compression artifacts in virtual pathology images. IEEE Trans. Med. Imaging 2011, 30, 306–314. [Google Scholar] [CrossRef] [Green Version]
- Singh, N.; Kaur, L.; Singh, K. Histogram equalization techniques for enhancement of low radiance retinal images for early detection of diabetic retinopathy. Eng. Sci. Technol. Int. J. 2019, 22, 736–745. [Google Scholar] [CrossRef]
- Al-Ameen, Z. Expeditious contrast enhancement for grayscale images using a new swift algorithm. Stat. Optim. Inf. Comput. 2018, 6. [Google Scholar] [CrossRef] [Green Version]
- Wong, C.Y.; Liu, S.; Liu, S.C.; Rahman, M.A.; Lin, S.C.-F.; Jiang, G.; Kwok, N.; Shi, H. Image contrast enhancement using histogram equalization with maximum intensity coverage. J. Mod. Opt. 2016, 63, 1618–1629. [Google Scholar] [CrossRef]
- Singh, K.; Vishwakarma, D.K.; Walia, G.S.; Kapoor, R. Contrast enhancement via texture region based histogram equalization. J. Mod. Opt. 2016, 63, 1444–1450. [Google Scholar] [CrossRef]
- Singh, K.; Kapoor, R. Image enhancement via median-mean based sub-image-clipped histogram equalization. Optik 2014, 125, 4646–4651. [Google Scholar] [CrossRef]
- Rahman, S.; Rahman, M.M.; Abdullah-Al-Wadud, M.; Al-Quaderi, G.D.; Shoyaib, M. An adaptive gamma correction for image enhancement. EURASIP J. Image Video Process. 2016, 2016, 35. [Google Scholar] [CrossRef] [Green Version]
- Jiang, G.; Wong, C.Y.; Lin, S.C.F.; Rahman, M.A.; Ren, T.R.; Kwok, N.; Shi, H.; Yu, Y.-H.; Wu, T. Image contrast enhancement with brightness preservation using an optimal gamma correction and weighted sum approach. J. Mod. Opt. 2015, 62, 536–547. [Google Scholar] [CrossRef]
- Singh, K.; Kapoor, R.; Sinha, S.K. Enhancement of low exposure images via recursive histogram equalization algorithms. Optik 2015, 126, 2619–2625. [Google Scholar] [CrossRef]
- Huang, S.-C.; Cheng, F.-C.; Chiu, Y.-S. Efficient contrast enhancement using adaptive gamma correction with weighting distribution. IEEE Trans. Image Process. 2013, 22, 1032–1041. [Google Scholar] [CrossRef]
- Singh, K.; Kapoor, R. Image enhancement using Exposure based Sub Image Histogram Equalization. Pattern Recognit. Lett. 2014, 36, 10–14. [Google Scholar] [CrossRef]
- Siracusano, G.; La Corte, A.; Gaeta, M.; Finocchio, G. A data-oriented self-calibration and robust chemical-shift encoding by using clusterization (OSCAR): Theory, optimization and clinical validation in neuromuscular disorders. Magn. Reson. Imaging 2018, 45. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ENT | CII | |
|---|---|---|
| AGCWD [77] | 6.94 +/− 0.62 | 1.27 +/− 0.33 |
| CEGAMMA [75] | 6.84 +/− 0.64 | 0.94 +/− 0.07 |
| ESIHE [78] | 6.86 +/− 0.63 | 1.11 +/− 0.18 |
| MMSICHE [73] | 6.85 +/− 0.63 | 1.05 +/− 0.1 |
| R-ESIHE [76] | 6.77 +/− 0.62 | 1.09 +/− 0.21 |
| RS-ESIHE [76] | 6.72 +/− 0.65 | 0.9 +/− 0.23 |
| DOTHE [72] | 6.46 +/− 0.59 | 1.23 +/− 0.29 |
| CLAHE [38] | 7.27 +/− 0.57 | 1.18 +/− 0.17 |
| PACE | * 7.69 +/− 0.2 | * 1.31 +/− 0.24 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siracusano, G.; La Corte, A.; Gaeta, M.; Cicero, G.; Chiappini, M.; Finocchio, G. Pipeline for Advanced Contrast Enhancement (PACE) of Chest X-ray in Evaluating COVID-19 Patients by Combining Bidimensional Empirical Mode Decomposition and Contrast Limited Adaptive Histogram Equalization (CLAHE). Sustainability 2020, 12, 8573. https://doi.org/10.3390/su12208573
Siracusano G, La Corte A, Gaeta M, Cicero G, Chiappini M, Finocchio G. Pipeline for Advanced Contrast Enhancement (PACE) of Chest X-ray in Evaluating COVID-19 Patients by Combining Bidimensional Empirical Mode Decomposition and Contrast Limited Adaptive Histogram Equalization (CLAHE). Sustainability. 2020; 12(20):8573. https://doi.org/10.3390/su12208573
Chicago/Turabian StyleSiracusano, Giulio, Aurelio La Corte, Michele Gaeta, Giuseppe Cicero, Massimo Chiappini, and Giovanni Finocchio. 2020. "Pipeline for Advanced Contrast Enhancement (PACE) of Chest X-ray in Evaluating COVID-19 Patients by Combining Bidimensional Empirical Mode Decomposition and Contrast Limited Adaptive Histogram Equalization (CLAHE)" Sustainability 12, no. 20: 8573. https://doi.org/10.3390/su12208573