
Dietary Therapy to Improve Nutrition and Gut Health in Paediatric Crohn’s Disease; A Feasibility Study
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Public and Public Involvement
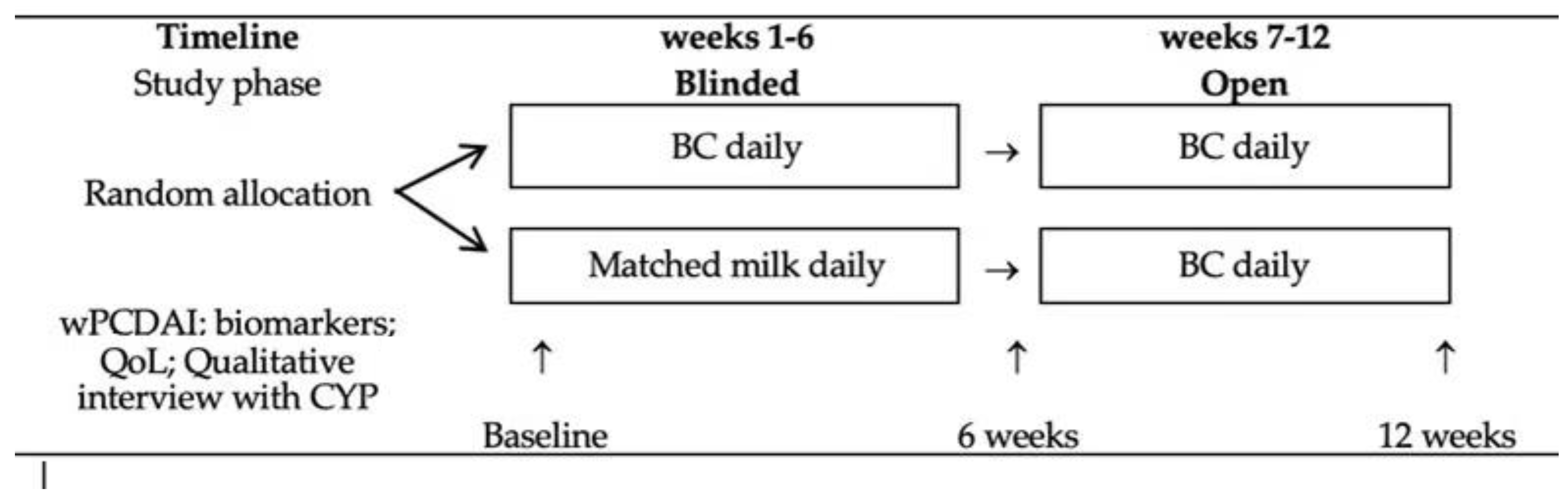
2.2. Intervention Trial
2.3. Statistical Methods
3. Results
3.1. Adherence with Trial Procedures and Milk Products
3.2. Clinical Outcomes
3.3. Laboratory Outcomes
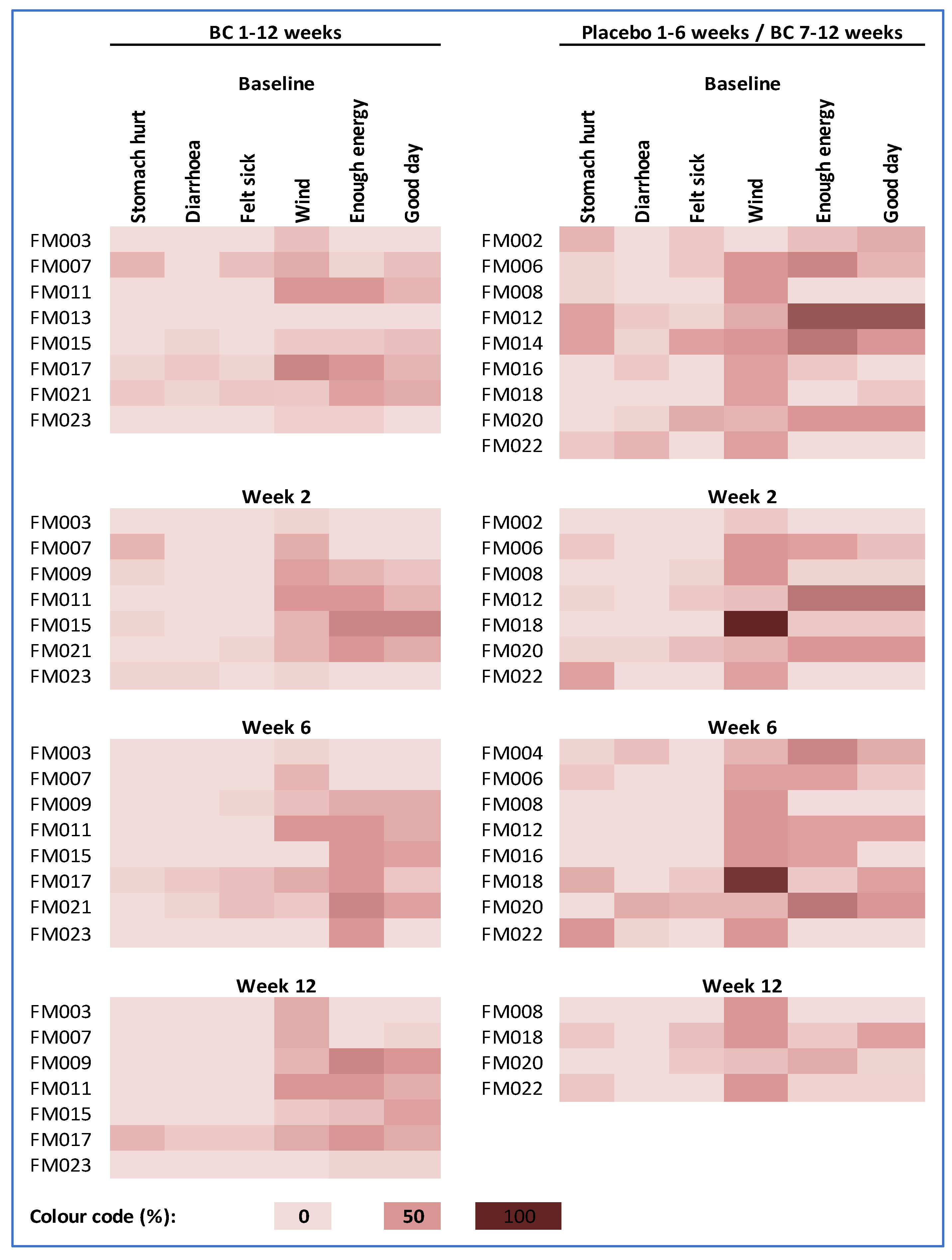
3.4. Qualitative Findings
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Trial registration
Appendix A. Impact–III Questionnaire (UK)
Instructions
| ☐ Not at all | ☐ A little | ☐ Quite a bit | ☐ Much | ☐ Very much |
| ☐ Not at all | ☐ A little | ☐ Quite a bit | ☐ Much | ☐ Very much |
| ☐ Not at all | ☐ A little | ☐ Quite a bit | ☐ Much | ☐ Very much |
| ☐ Not at all | ☐ A little | ☐ Quite a bit | ☐ Much | ☐ Very much |
| ☐ Not at all | ☐ A little | ☐ Quite a bit | ☐ Much | ☐ Very much |
| ☐ Very much energy | ☐ Much energy | ☐ Quite a bit of energy | ☐ A little energy | ☐ No energy at all |
| ☐ I feel great about my weight | ☐ I feel good about my weight | ☐ I don’t feel good or bad about my weight | ☐ I feel bad about my weight | ☐ I feel awful about my weight |
| ☐ The effect has been great | ☐ The effect has been good | ☐ It has not affected our family | ☐ The effect has been bad | ☐ The effect has been awful |
| ☐ Never | ☐ Rarely | ☐ Sometimes | ☐ Often | ☐ Very often |
| ☐ Never | ☐ Rarely | ☐ Sometimes | ☐ Often | ☐ Very often |
| ☐ Not at all | ☐ A little | ☐ Quite a bit | ☐ Much | ☐ Very much |
| ☐ Never | ☐ Rarely | ☐ Sometimes | ☐ Often | ☐ Very often |
| ☐ Never | ☐ Rarely | ☐ Sometimes | ☐ Often | ☐ Very often |
| ☐ Not at all | ☐ A little | ☐ Quite a bit | ☐ Much | ☐ Very much |
| ☐ I think I look great | ☐ I think I look good | ☐ I don’t think I look good or bad | ☐ I think I look bad | ☐ I think I look awful |
| ☐ Not at all | ☐ A little | ☐ Quite a bit | ☐ Much | ☐ Very much |
| ☐ Not at all | ☐ A little | ☐ Quite a bit | ☐ Much | ☐ Very much |
| ☐ Not at all | ☐ A little | ☐ Quite a bit | ☐ Much | ☐ Very much |
| ☐ Never | ☐ Rarely | ☐ Sometimes | ☐ Often | ☐ Very often |
| ☐ Not at all | ☐ A little | ☐ Quite a bit | ☐ Much | ☐ Very much |
| ☐ Never | ☐ Rarely | ☐ Sometimes | ☐ Often | ☐ Very often |
| ☐ I do not mind them at all | ☐ I mind them a tiny bit | ☐ I mind them a little | ☐ I mind them a lot | ☐ I hate them |
| ☐ Never | ☐ Rarely | ☐ Sometimes | ☐ Often | ☐ Very often |
| ☐ Never | ☐ Rarely | ☐ Sometimes | ☐ Often | ☐ Very often |
| ☐ Never | ☐ Rarely | ☐ Sometimes | ☐ Often | ☐ Very often |
| ☐ No, I do not try at all | ☐ I don’t try much | ☐ I try a little | ☐ I try hard | ☐ Yes, I try very hard |
| ☐ No, not difficult | ☐ Slightly difficult | ☐ Quite difficult | ☐ Very difficult | ☐ Yes, extremely difficult |
| ☐ Great | ☐ Good | ☐ Not good or bad | ☐ Bad | ☐ Awful |
| ☐ Yes, very happy | ☐ Happy | ☐ Not happy or unhappy | ☐ Unhappy | ☐ Very unhappy |
| ☐ Always | ☐ Often | ☐ Sometimes | ☐ Rarely | ☐ Never |
| ☐ Never | ☐ Rarely | ☐ Sometimes | ☐ Often | ☐ Very often |
| ☐ Not at all tired | ☐ A little tired | ☐ Quite tired | ☐ Tired | ☐ Very tired |
| ☐ I feel great about my height | ☐ I feel good about my height | ☐ I don’t feel good or bad about my height | ☐ I feel bad about my height | ☐ I feel awful about my height |
| ☒ Yes, as much as I would like | ☐ Almost as much as I would like | ☐ About half as much as I would like | ☐ Less than half as much as I would like | ☐ Much less than I would like |
| ☐ Always | ☐ Often | ☐ Sometimes | ☐ Rarely | ☐ Never |
References
- Torres, J.; Mehandru, S.; Colombel, J.F.; Peyrin-Biroulet, L. Crohn’s disease. Lancet 2017, 389, 1741–1755. [Google Scholar] [CrossRef]
- Benchimol, E.I.; Fortinsky, K.J.; Gozdyra, P.; Van den Heuvel, M.; Van Limbergen, J.; Griffiths, A.M. Epidemiology of pediatric inflammatory bowel disease: A systematic review of international trends. Inflamm. Bowel Dis. 2011, 17, 423–439. [Google Scholar] [CrossRef]
- van Rheenen, P.F.; Aloi, M.; Assa, A.; Bronsky, J.; Escher, J.C.; Fagerberg, U.L.; Gasparetto, M.; Gerasimidis, K.; Griffiths, A.; Henderson, P.; et al. The Medical Management of Paediatric Crohn’s Disease: An ECCO-ESPGHAN Guideline Update. J. Crohn′s Colitis 2020, 15, 171–194. [Google Scholar] [CrossRef] [PubMed]
- Cameron, F.L.; Gerasimidis, K.; Papangelou, A.; Missiou, D.; Garrick, V.; Cardigan, T.; Buchanan, E.; Barclay, A.R.; McGrogan, P.; Russell, R.K. Clinical progress in the two years following a course of exclusive enteral nutrition in 109 paediatric patients with Crohn’s disease. Aliment. Pharmacol. Ther. 2013, 37, 622–629. [Google Scholar] [CrossRef]
- Day, A.S.; Whitten, K.E.; Sidler, M.; Lemberg, D.A. Systematic review: Nutritional therapy in paediatric Crohn’s disease. Aliment. Pharmacol. Ther. 2008, 27, 293–307. [Google Scholar] [CrossRef] [PubMed]
- Hoekman, D.R.; Diederen, K.; Koot, B.G.; Tabbers, M.M.; Kindermann, A.; Benninga, M.A. Relationship of clinical symptoms with biomarkers of inflammation in pediatric inflammatory bowel disease. Eur. J. Pediatr. 2016, 175, 1335–1342. [Google Scholar] [CrossRef] [Green Version]
- Frivolt, K.; Schwerd, T.; Werkstetter, K.J.; Schwarzer, A.; Schatz, S.B.; Bufler, P.; Koletzko, S. Repeated exclusive enteral nutrition in the treatment of paediatric Crohn’s disease: Predictors of efficacy and outcome. Aliment. Pharmacol. Ther. 2014, 39, 1398–1407. [Google Scholar] [CrossRef]
- El-Matary, W.; Otley, A.; Critch, J.; Abou-Setta, A.M. Enteral Feeding Therapy for Maintaining Remission in Crohn’s Disease: A Systematic Review. J. Parenter. Enter. Nutr. (JPEN) 2017, 41, 550–561. [Google Scholar] [CrossRef]
- Hansen, T.; Duerksen, D.R. Enteral Nutrition in the Management of Pediatric and Adult Crohn’s Disease. Nutrients 2018, 10, 537. [Google Scholar] [CrossRef] [Green Version]
- Kansal, S.; Wagner, J.; Kirkwood, C.D.; Catto-Smith, A.G. Enteral nutrition in Crohn’s disease: An underused therapy. Gastroenterol. Res. Pract. 2013, 2013, 482108. [Google Scholar] [CrossRef]
- Aloi, M.; Nuti, F.; Stronati, L.; Cucchiara, S. Advances in the medical management of paediatric IBD. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Playford, R.J.; Weiser, M.J. Bovine Colostrum: Its Constituents and Uses. Nutrients 2021, 13, 265. [Google Scholar] [CrossRef] [PubMed]
- Chandwe, K.; Kelly, P. Colostrum Therapy for Human Gastrointestinal Health and Disease. Nutrients 2021, 13, 1956. [Google Scholar] [CrossRef]
- Turner, D.; Griffiths, A.M.; Walters, T.D.; Seah, T.; Markowitz, J.; Pfefferkorn, M.; Keljo, D.; Waxman, J.; Otley, A.; LeLeiko, N.S.; et al. Mathematical weighting of the pediatric Crohn’s disease activity index (PCDAI) and comparison with its other short versions. Inflamm. Bowel Dis. 2012, 18, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Uggla, C.; Lindh, V.; Lind, T.; Lindkvist, M. IMPACT-III is a valid and reliable questionnaire for assessing health-related quality of life in Swedish children with inflammatory bowel disease. Acta Paediatr. 2018, 107, 347–353. [Google Scholar] [CrossRef]
- James Lind Alliance. 2013. Available online: https://www.jla.nihr.ac.uk/priority-setting-partnerships/inflammatory-bowel-disease/top-10-priorities/ (accessed on 25 September 2022).
- Wilschanski, M.; Sherman, P.; Pencharz, P.; Davis, L.; Corey, M.; Griffiths, A. Supplementary enteral nutrition maintains remission in paediatric Crohn’s disease. Gut 1996, 38, 543–548. [Google Scholar] [CrossRef]
- Duncan, H.; Buchanan, E.; Cardigan, T.; Garrick, V.; Curtis, L.; McGrogan, P.; Barclay, A.; Russell, R.K. A retrospective study showing maintenance treatment options for paediatric CD in the first year following diagnosis after induction of remission with EEN: Supplemental enteral nutrition is better than nothing! BMC Gastroenterol. 2014, 14, 50. [Google Scholar] [CrossRef] [Green Version]
- Levine, A.; Wine, E.; Assa, A.; Sigall Boneh, R.; Shaoul, R.; Kori, M.; Cohen, S.; Peleg, S.; Shamaly, H.; On, A.; et al. Crohn’s Disease Exclusion Diet Plus Partial Enteral Nutrition Induces Sustained Remission in a Randomized Controlled Trial. Gastroenterology 2019, 157, 440–450.e8. [Google Scholar] [CrossRef] [Green Version]
- Johnson, T.; Macdonald, S.; Hill, S.M.; Thomas, A.; Murphy, M.S. Treatment of active Crohn’s disease in children using partial enteral nutrition with liquid formula: A randomised controlled trial. Gut 2006, 55, 356–361. [Google Scholar] [CrossRef] [Green Version]
- Svolos, V.; Gerasimidis, K.; Buchanan, E.; Curtis, L.; Garrick, V.; Hay, J.; Laird, S.; Munro, J.; Gaya, D.R.; Russell, R.K.; et al. Dietary treatment of Crohn’s disease: Perceptions of families with children treated by exclusive enteral nutrition, a questionnaire survey. BMC Gastroenterol. 2017, 17, 14. [Google Scholar] [CrossRef]
- Mehra, R.; Garhwal, R.; Sangwan, K.; Guiné, R.P.F.; Lemos, E.T.; Buttar, H.S.; Visen, P.K.S.; Kumar, N.; Bhardwaj, A.; Kumar, H. Insights into the Research Trends on Bovine Colostrum: Beneficial Health Perspectives with Special Reference to Manufacturing of Functional Foods and Feed Supplements. Nutrients 2022, 14, 659. [Google Scholar] [CrossRef] [PubMed]
- Slonim, A.E.; Grovit, M.; Bulone, L. Effect of exclusion diet with nutraceutical therapy in juvenile Crohn’s disease. J. Am. Coll. Nutr. 2009, 28, 277–285. [Google Scholar] [CrossRef]
- Khan, Z.; Macdonald, C.; Wicks, A.C.; Holt, M.P.; Floyd, D.; Ghosh, S.; Wright, N.A.; Playford, R.J. Use of the ‘nutriceutical’, bovine colostrum, for the treatment of distal colitis: Results from an initial study. Aliment. Pharmacol. Ther. 2002, 16, 1917–1922. [Google Scholar] [CrossRef] [PubMed]
- Playford, R.J.; Cattell, M.; Marchbank, T. Marked variability in bioactivity between commercially available bovine colostrum for human use; implications for clinical trials. PLoS ONE 2020, 15, e0234719. [Google Scholar] [CrossRef]
- Playford, R.J. The Use of Bovine Colostrum in Medical Practice and Human Health: Current Evidence and Areas Requiring Further Examination. Nutrients 2021, 14, 92. [Google Scholar] [CrossRef]
- Montrose, D.C.; Nishiguchi, R.; Basu, S.; Staab, H.A.; Zhou, X.K.; Wang, H.; Meng, L.; Johncilla, M.; Cubillos-Ruiz, J.R.; Morales, D.K.; et al. Dietary Fructose Alters the Composition, Localization, and Metabolism of Gut Microbiota in Association With Worsening Colitis. Cell. Mol. Gastroenterol. Hepatol. 2021, 11, 525–550. [Google Scholar] [CrossRef]
- Ritchie, J.; Spencer, L. Qualitative data analysis for applied policy research. In Analyzing Qualitative Data; Bryman, A., Burgess, R.G., Eds.; Routledge: London, UK, 1994; pp. 173–194. [Google Scholar]
- Gale, N.K.; Heath, G.; Cameron, E.; Rashid, S.; Redwood, S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med. Res. Methodol. 2013, 13, 117. [Google Scholar] [CrossRef] [Green Version]
- Playford, R.J.; MacDonald, C.E.; Calnan, D.P.; Floyd, D.N.; Podas, T.; Johnson, W.; Wicks, A.C.; Bashir, O.; Marchbank, T. Co-administration of the health food supplement, bovine colostrum, reduces the acute non-steroidal anti-inflammatory drug-induced increase in intestinal permeability. Clin. Sci. (Lond.) 2001, 100, 627–633. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| First Milk N = 12 | Placebo N = 11 | |
|---|---|---|
| Demographic variables | ||
| Age (median, IQR; months) | 15.4 (13.4–16.4) | 14.9 (13.9–16.0) |
| Female (No; %) | 5 (41.7) | 4 (36.4) |
| Ethnicity White British (No; %) | 11 (91.7%) | 9 (81.8%) |
| Clinical Variables | ||
| Age at diagnosis (median, IQR; years) | 12.3 (8.9–14.4) | 11.9 (9.6–14.3) |
| Height 1 (median, IQR; m) | 161.8 (149.8–170.4) | 164.5 (155.8–171.9) |
| Weight 1 (median, IQR; kg) | 57.4 (49.6–61.6) | 53.2 (43.0–63.2) |
| Disease location 2 (No; %) | ||
| 0 (0.0) | 1 (9.1) |
| 2 (16.7) | 3 (27.3) |
| 7 (58.3) | 7 (63.3) |
| 0 (0.0) | 1 (9.1) |
| 2 (16.7) | 2 (18.2) |
| Disease behaviour (No; %) | ||
| 9 (66.7) | 9 (81.8) |
| 0 (0.0) | 1 (9.1) |
| 1 (8.3) | 0 (0.0) |
| 5 (41.7) | 3 (27.3) |
| Growth delay (height for age Z score < −1.64) (No; %) | 0 (0.0) | 1 (9.1) |
| Disease activity 3 (No; %) | ||
| 8 (72.7) | 7 (70.0) |
| 3 (30.0) | 3 (27.3) |
| 0.0 (0.0–25.0) | 7.5 (5.0–30.0) |
| Extra-intestinal manifestations 4 (No; %) | ||
| 4 (40.0) | 2 (18.2) |
| 3 (30.0) | 3 (27.3) |
| 1 (10.0) | 0 (0.0) |
| 2 (20.0) | 2 (18.2) |
| 0 (0.0) | 0 (0.0) |
| 4 (40.0) | 4 (36.4) |
| 1 (10.0) | 1 (9.1) |
| 1 (10.0) | 0 (0.0) |
| Current treatment 5 (No; %) | ||
| 1 (10.0) | 1 (9.1) |
| 5 (50.0) | 7 (63.6) |
| 7 (70.0) | 9 (81.8) |
| Past medical history (No; %) | ||
| 3 (25.0) | 3 (27.3) |
| 1 (8.3) | 0 (0.0) |
| 1 (8.3) | 0 (0.0) |
| 0 (0.0) | 1 (9.1) |
| 0 (0.0) | 1 (9.1) |
| 0 (0.0) | 1 (9.1) |
| 0 (0.0) | 1 (9.1) |
| Quality of life 6 (No.; median; IQR) | 63.0 (49.0–82.0) | 63.5 (59.0–74.0) |
| Clinical Variable | Change Weeks 1–6 No. Median (IQR) | p Value | Change Weeks 1–12 No. Median (IQR) | Change in All Children after 6 Weeks BC No. Median (IQR) | |
|---|---|---|---|---|---|
| BC | Placebo | BC | BC | ||
| Disease actvity 1 | 7 −10 (−15.0–5.0) | 10 −1.25 (−13.1–13.1) | 1.0 | 4 −15.0 (−28.8–−1.25) | 12 −2.5 (−13.75–4.38) |
| Height (cm) | 9 0.7 (−0.45–1.6) | 10 1.0 (0.075–2.4) | 0.07 | 8 0.7 (−0.13–1.68) | 13 0.5 (−0.55–1.55) |
| Weight (kg) | 9 1.2 (−0.5–3.2) | 10 1.6 (−0.74–2.48) | 0.37 | 8 1.55 (−1.24–2.98) | 13 0.5 (−0.55–1.5) |
| Quality of life 2 | 6 −1.5 (−10.0–1.0) | 9 −12.0 (−15.0–−4.0) | 0.15 | 4 −12.5 (−17.8–−2.8) | 11 0.0 (−7.0–4.0) |
| Biomarker/Variable | Baseline No. Median (IQR) | Change Weeks 1–6 No. Median (IQR) | p Value | Change Weeks 1–12; FM Group No. Median (IQR) | Change in All Children after 6 Weeks FM No. Median (IQR) | ||
|---|---|---|---|---|---|---|---|
| First Milk | Placebo | First Milk | Placebo | ||||
| Intestinal inflammation | |||||||
| Faecal calprotectin (μg/g stool) Normal <50 μg/g stool | 8 23.5 (14.5 to 60.3) | 7 80.0 (10.0 to 532.0) | 7 −9.0 (−14.0 to 61.0) | 6 −45.5 (−322.8 to −0.5) | 0.59 | 7 −1.0 (−14.1 to 724.0) | 12 −10.05 (−35.5 to 2.25) |
| Mucosal integrity | |||||||
| Faecal alpha 1–antitrypsin (mg/dl) Normal <26.8 mg/dl | 7 31.2 (11.7 to 40.4) | 8 13.4 (7.7–175.3) | 6 −11.9 (−29.0 to 1.74) | 7 5.11 (0.00 to 10.1) | 0.10 | 6 −17.3 (−31.4 to −4.13) | 11 −2.86 (−20.9 to 12.6) |
| Plasma intestinal fatty acid binding protein (pg/mL) Normal range 230–1800 pg/mL | 11 746.0 (352.4 to 1494.5) | 10 521.0 (360.3 to 695.8) | 8 −257.6 (−633.3 to 115.6) | 9 94.2 (−21.0 to 245.1) | 0.15 | 8 −23.9 (−473.0 to 515.5) | 13 75.9 (−329.6 to 261.5) |
| Plasma anti-IgA endotoxin (AMU/mL) | 11 50.6 (31.2 to 70.1) | 10 25.8 (19.3 to 74.4) | 8 −0.2 (−15.8 to 4.1) | 9 −1.24 (−11.3 to 4.02) | 1.0 | 8 0.93 (−9.87 to 18.8) | 13 −0.46 (−12.7 to 3.89) |
| Plasma anti-IgG endotoxin (GMU/mL) | 11 118.3 (64.7 to 127.7) | 10 53.6 (29.6 to 138.8) | 8 35.3 (−56.6 to 99.7) | 9 −6.3 (−56.6 to 40.0) | 0.35 | 8 −10.8 (−22.3 to 29.1) | 13 14.6 (−26.0 to 91.1) |
| Plasma anti-IgM endotoxin (MMU/mL) | 11 110.8 (86.3 to 161.4) | 10 65.0 (48.9 to 115.7) | 8 −0.48 (−20.5 to 42.6) | 9 1.3 (−3.67 to 16.4) | 1.0 | 8 5.55 (−19.7 to 25.2) | 13 −1.97 (−18.6 to 17.9) |
| Urine sugar permeability test (ratio of % recovery lactulose/rhamnose) | 10 0.030 (0.021 to 0.044) | 10 0.030 (0.026 to 0.045) | 8 −0.0046 (−0.0064 to 0.012) | 9 −0.0046 (−0.014 to 0.0047) | 1.0 | 8 0.0021 (−0.020 to 0.015) | 13 0.0033 (−0.0059 to 0.011) |
| Systemic inflammation | |||||||
| Plasma C-reactive protein (mg/L) Normal range 0.11–4.52 mg/L | 11 3.90 (3.90 to 4.00) | 10 4.00 (3.90 to 4.73) | 8 0.0 (0.0 to 0.08) | 9 0.0 (0.0 to 0.0) | 0.21 | 8 0.0 (−1.0 to 0.0) | 13 0.0 (−0.05 to 0.0) |
| Plasma alpha 1 acid glycoprotein (μg/mL) Normal range 286–1087 μg/ml | 11 1002.0 (599.2 to 1501.5) | 10 814.2 (575.1 to 967.4) | 8 78.2 (−66.3 to 230.9) | 9 42.0 (−369.4 to 376.9) | 1.0 | 8 −6.4 (−220.6 to 253.1) | 13 −93.6 (−937.3 to 109.4) |
| Growth factors | |||||||
| Insulin-like growth factor−1 (ng/mL) Normal range 43–182 ng/ml | 11 244.2 (169.5 to 312.8) | 10 264.6 (237.6 to 283.6) | 8 9.95 (−68.1 to 48.6) | 9 −3.77 (−27.3 to 27.7) | 1.0 | 8 9.3 (−55.0 to 19.9) | 13 38.0 (−36.4 to 47.72) |
| Insulin-like growth factor binding protein−3 (ng/mL) Normal range 1553–3089 ng/ml | 11 2550.4 (2238.4 to 3017.1) | 10 2624.6 (2506.6 to 3104.9) | 8 −9.09 (−42.6 to 236.9) | 9 144.4 (−252.0 to 284.4) | 0.153 | 8 74.7 (−338.7 to 497.5) | 13 39.96 (−37.1 to 507.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Allen, S.J.; Belnour, S.; Renji, E.; Carter, B.; Bray, L.; Allen, A.; Jones, E.; Urban, B.; Moule, S.; Wang, D.; et al. Dietary Therapy to Improve Nutrition and Gut Health in Paediatric Crohn’s Disease; A Feasibility Study. Nutrients 2022, 14, 4598. https://doi.org/10.3390/nu14214598
Allen SJ, Belnour S, Renji E, Carter B, Bray L, Allen A, Jones E, Urban B, Moule S, Wang D, et al. Dietary Therapy to Improve Nutrition and Gut Health in Paediatric Crohn’s Disease; A Feasibility Study. Nutrients. 2022; 14(21):4598. https://doi.org/10.3390/nu14214598
Chicago/Turabian StyleAllen, Stephen J., Salma Belnour, Elizabeth Renji, Bernie Carter, Lucy Bray, Angela Allen, Emma Jones, Britta Urban, Sarah Moule, Duolao Wang, and et al. 2022. "Dietary Therapy to Improve Nutrition and Gut Health in Paediatric Crohn’s Disease; A Feasibility Study" Nutrients 14, no. 21: 4598. https://doi.org/10.3390/nu14214598